

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mupirocin is a topical antibiotic that was originally isolated from Pseudomonas fluorescens, and it inhibits bacterial protein synthesis by competitively binding to isoleucyl-tRNA synthetase (IleS). This drug is particularly effective against streptococci and staphylococci, including methicillin-resistant Staphylococcus aureus (MRSA). Mupirocin is one of the most popular topical agents used for the treatment of skin infection and eradication of nasal carriage of MRSA1. The increased use of this antibiotic has been accompanied by outbreaks of MRSA that are resistant to mupirocin2.
The mupirocin resistant strains are divided into two groups depending on the minimum inhibitory concentration (MIC) against mupirocin: low-level resistance (MIC=8~256µg/ml) and high-level resistance (MIC>256µg/ml). High-level mupirocin resistant strains are important in the clinical field because they are able to transfer resistance genes to other bacteria by plasmid conjugation, consequently protecting these bacteria from being eradicated with mupirocin3.
MATERIALS AND METHODS
Bacterial isolates
A total of 193 MRSA isolates were collected from the clinical cultures taken from patients at four Korean university hospitals (A~D) from April 2008 to July 2009. The specimens originated from the skin, pus, blood, central venous catheter tip, sputum, tracheal tip, urine, and wound. Of these, 103 strains were from (A) hospital and 30 strains were from the other 3 hospitals, respectively. All the MRSA isolates were randomly collected from each of the hospitals.
Antimicrobial susceptibility test
The susceptibility to antimicrobial agents was determined by agar dilution tests, according to the guidelines provided by the Clinical and Laboratory Standards Institute (CLSI). Eight antimicrobial agents were tested: ciprofloxacin, clindamycin, erythromycin, fusidic acid, mupirocin, rifampin, tetracycline and vancomycin. S. aureus ATCC 33591 was used as a control strain.
Briefly, serial two-fold dilutions of the antibiotics were prepared in Muller-Hinton agar (Difco Laboratories, Detroit, MI, USA). The strains were subcultured on tryptic soy agar (Difco Laboratories), suspended in tryptic soy broth (Difco Laboratories) and adjusted to the turbidity of a 0.5 McFarland standard. Next, the suspension was diluted 1:10 and inoculated on each plate coated with antibiotic containing media by a Steer replicator. The inoculated plates were incubated at 35℃ for 24 hr. The lowest concentration of antibiotic that inhibits the visible growth of an organism was regarded as the MIC, and growth of one isolate was ignored. The MIC50 and MIC90 were the MICs that were required to inhibit 50% and 90% of the organisms, respectively. The MIC determination was evaluated according to the CLSI guidelines7.
Detection of the femA, mecA and mupA genes by polymerase chain reaction (PCR)
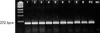
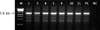
All the isolates were confirmed to be S. aurues and MRSA by detection of the femA and mecA genes using a PCR assay. The high level mupirocin resistant strains were also confirmed by detection of the mupA gene (Fig. 1, 2, 3, 4). Three primer pairs were used for the detection of the femA, mecA and mupA genes. For femA gene detection, forward primer (5'-CATGATGGCGAGATTACAGG-3') and reverse primer (5'-CGCTAAAGGTACTAACACACGG-3') with a fragment of 372 bp were used8. For mecA gene detection, forward primer (5'-ATGAGATTAGGCATCGTTCC-3') and reverse primer (5'-TGGATGACAGTACCTGAGCC-3') with a fragment of 554 bp were used9. For mupA gene detection, forward primer (5'-CCCATGGCTTACCAGTTGA-3') and reverse primer (5'-CCATGGAGCACTATCCGAA-3') with a fragment of 1.6 kb were used10.
Prior to DNA extraction, frozen bacteria were subcultured twice onto Mueller-Hinton agar plates. For extraction, one to five bacterial colonies were suspended in 50µl of cell lysis buffer (Genotek Co., Daejeon, Korea) and this was heated at 100℃ for 10 min. After centrifugation at 12,000 rpm for 10 min, 2µl of the supernatant was used for DNA extraction. The PCR reactions were performed using a Primer Mix Kit (Genotek Co.). The thermal cycler (GeneAmp PCR system 9700, Perkin-Elmer Cetus, Foster City, CA, USA) was programmed with the following parameters: pre-denaturation at 95℃ for 15 min, 30 cycles of denaturation at 94℃ for 30 s, annealing at 68℃ for 90 s, extension at 72℃ for 90 s and a final extension at 72℃ for 10 min. The amplified products were run on a 2% agarose gel for 20 min at 200 volts and visualized with ethidium bromide.
Pulsed-field gel electrophoresis (PFGE)
A total of 16 strains of mupirocin resistant MRSA (10 isolates with high-level resistance and 6 isolates with low-level resistance) were used for PFGE11. The high-level resistant strains were from (A) hospital. For the low-level strains, 2 strains were from (B) hospital, 3 strains were from (C) hospital and one strain was from (D) hospital.
Each isolate was inoculated into 3 ml Luria-Vertani broth (Difco Laboratories) and incubated at 37℃ overnight. The concentration of the cell suspensions were adjusted with saline using a spectrophotometer to an absorbance of 0.3~0.25 at 610 nm. After adjustment, 1 ml of the cell suspension was centrifuged at 14,000 rpm for 5 min and the supernatant was aspirated. The pellet was washed once in 1 ml of Tris-EDTA (TE) buffer (10 mM Tris HCl, 1 mM EDTA [pH 8]) and centrifuged again. The washed cells were resuspended in 50µl of lysis II buffer (6 mM Tris-HCl, pH 8.0, 1 M NaCl, 100 mM EDTA, 0.5% Brij-58, 0.2% sodium deoxycholate, 0.5% sodium lauroylsarcosine) and equilibrated at 37℃ for 15 min. Fifty microliters of 2% low-melting-pint agarose and 2µl of 100 units lysostaphin were added to the cell suspension, gently mixed and dispensed into a plug mold. The plugs were allowed to solidify in the refrigerator at 4℃ for 5 min. The plugs were placed into a tube containing 250µl of lysis I buffer (50 mM Tris-HCl, pH 7.4, 100 unit lysostapin, lysozyme 1 mg/ml) and the cells in the plug were lysed for 1 h at 37℃. Then the lysis I buffer were removed and replaced with 250µl of lysis II buffer at 37℃ for 1 h. The lysis II buffer was removed and 250µl of proteinase K buffer (0.5 M EDTA, 25 unit/ml proteinase K) was added and this was incubated at 50℃ overnight. The TE washings were repeated 3 more times.
For electrophoresis, the plug was cut into small slices (2 by 5 mm) and these were placed in 125µl of a total restriction enzyme mixture that contained 20 U of SmaI (Sib Enzyme Ltd, Novosibirk, Russia). After 2 h incubation at 25℃ with shaking at 140 rpm, the chromosomal restriction fragment patterns were analyzed by loading the trimmed slices of the plug into a well of SeaKem 1% agarose gel. The running gel was prepared in 0.5×TBE buffer (Bio-Rad Laboratories, Inc., Hercules, CA, USA). Electrophoresis was performed with a CHEP-DR III (Bio-Rad Laboratories, Inc., Hercules, CA, USA). The running parameters were an initial pulse of 5 s, a final pulse of 40 s, 200 V, 20 hrs and 12~14℃. After the electrophoresis run was completed, the gel was stained with 0.5µg/ml ethidium bromide for 20 min and destained in fresh distilled water for 20 min.
The gels were photographed and digitalized with a GelDoc (Bio-Rad Laboratories, Inc., Hercules, CA, USA). The images were stored electronically as TIFF files. The restriction pattern was analyzed with the GelCompar II program (version 4.5; Applied Maths, Sint-Martens-Latem, Belgium) using the Dice coefficient, and cluster analysis of the similarity matrices was performed by the unweighted pair group method using the arithmetic average with 0.75% of tolerance12,13. The similarity cut-off value was 99%.
RESULTS
Prevalence of mupirocin resistant MRSA
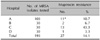
Of the total 193 clinical isolates of MRSA from the four university hospitals, 27 (14.1%) were mupirocin resistant (Table 1). Of these, 11 (5.7%) were found to have high-level resistance to mupirocin and all of them were from (A) hospital. The low-level strains were composed of 2, 13 and 1 isolates from (B), (C) and (D) hospitals, respectively.
Antimicrobial susceptibility tests of the mupirocin resistant MRSA
The antimicrobial susceptibility test results for the mupirocin resistant MRSA isolates are summarized in Table 2. The MICs of the high-level mupirocin resistant MRSA ranged from 512 to ≥1,024µg/ml, and the MIC50 and MIC90 were ≥1,024µg/ml, respectively. But for the low-level mupirocin resistant strains, the MICs ranged from 16 to 32, and the MIC50 and MIC90 was 16µg/ml in both cases. Compared with the MIC90 among the high-level resistant strains, rifampin and vancomycin showed high antimicrobial activity and the MICs were ≤0.5µg/ml and 0.5µg/ml, respectively. The MICs of ciprofloxacin and tetracycline were 64µg/ml, respectively and those for erythromycin and fusidic acid were ≥128µg/ml, respectively. For the low-level mupirocin resistant MRSA strains, vancomycin showed the highest antimicrobial activity (MIC=1µg/ml) and this was followed by rifampin (2µg/ml), tetracycline (32µg/ml) and ciprofloxacin (64µg/ml). The MICs of clindamycin, erythromycin and fusidic acid were ≥128µg/ml, respectively.
The high-level mupirocin resistant MRSA strains were susceptible to rifampin and vancomycin, but 90% were resistant to fusidic acid, and 100% were resistant to ciprofloxacin, clindamycin, tetracycline and erythromycin. While the low-level mupirocin resistant MRSA strains were susceptible to vancomycin, 6% were resistant to rifampin, 24% were resistant to erythromycin, 77% were resistant to fusidic acid and 100% were resistant to ciprofloxacin, clindamycin and tetracycline.
Genotyping the mupirocin resistant MRSA using the PFGE patterns
The PFGE patterns of the genomic DNA of the 16 strains of mupirocin resistant MRSA were classified into five clusters (Fig. 5). Of the 10 high-level resistant strains from (A) hospital, 9 (H1-H7, H9-H10) were classified in cluster 1 with 92% similarity. Among these, H6 and H10, H1-4 and H9, and H5 and H7 were the same clones. The H8 strain was in cluster 4 with 72% similarity. Of the 6 low-level resistant strains, L16-L18 from (B) hospital were classified in cluster 2 and they were the same clone with 100% similarity. The L19 and L20 from (A) hospital were in cluster 4 with 93% similarity, and L21 from (D) hospital was in cluster 5 with 79% similarity.
DISCUSSION
Mupirocin is a topical antibiotic that shows a high level of activity against streptococci and staphylococci, and certain gram-negative bacteria, including Haemophilus influenzae and Neisseria gonorrhoae, but it is much less active against most gram-negative bacilli and anaerobes1. Therefore, it has been used to treat skin infection and to eradicate MRSA. Mupirocin was introduced into clinical practice in 1985 and the use of mupirocin ointment has been progressively increasing worldwide.
Clinical isolates resistant to mupirocin were first reported in 1987, and the resistance rate has been increasing14. Prolonged use and frequent use of mupirocin were thought to be the most important factors associated with the increase of mupirocin resistance3,15. A Canadian study by Simor et al.2 reported an increase in mupirocin resistance among MRSA over time. From 1995 to 1999, the proportions of MRSA strains with high- and low-level mupirocin resistance were 1.6% and 6.4%, respectively, whereas from 2000 to 2004, the resistant rates were 7.0% and 10% respectively. Pérez-Fontán et al.16 reported the emergence of mupirocin-resistant S. aureus in peritoneal dialysis patients who applied mupirocin over 10 years. From 1990 to 1996, there were no mupirocin resistant strains, but they increased to 8.3% from 1997 to 1998, and to 12.4% from 1999 to 2000. According to Wise and Johnson17, the mupirocin resistance rate was 8.3% in a dermatological hospital, while it was 0.2% in the nearby general hospitals over the same period.
In Korea, topical mupirocin has been used since 1994 to eradicate staphylococcal infection in hospitals and the use of mupirocin has been dramatically increasing. However, there has been very little awareness and research about mupirocin resistance. The study conducted in Korea up to 1999 failed to detect mupirocin resistant strains18. Yet Yun et al.4 first identified 16 high-level mupirocin resistant isolates in 2003 and the prevalence of mupirocin resistance was 5%. In a study from long-term-care facilities in Korea, the rate of mupirocin resistance was 11.3% (6.1% high-level mupirocin resistance and 5.2% low-level mupirocin resistance)5. Another study carried out at intensive care units reported that the mupirocin resistance rate was 25.3% and all the isolates showed low-level resistance. In our study, the prevalence of mupirocin resistance was 14.1%. The 5.7% of the isolates were high-level resistant strains (11/193) and all of them were from (A) hospital. The low-level resistant strains were from the other three hospitals. Also, the prevalence of mupirocin resistance of (C) hospital was 43.3%, which is much higher than that of the other hospitals, and the reason for this was thought to be there were more dermatological samples from (C) hospital.
Mupirocin resistance is divided into two groups: low-level resistance (MIC=8~256µg/ml) and high-level resistance (MIC>256µg/ml). Low-level mupirocin resistance is due to point mutation in the chromosomally encoded native IleS gene, whereas high-level resistance is related to the acquisition of a plasmid containing a modified additional IleS-2 gene mupA3,4. However, the mupA gene was detected in the low-level mupirocin resistant strains by western blot analysis in a small case study10. It is also possible that high- and low-level mupirocin resistance are mediated by different, but closely related genes that hybridize with the mupA probe, so further studies are needed to resolve this issue.
Low-level mupirocin resistant strains are not considered to have clinical significance because the concentration of mupirocin in the 2% ointment (20,000µg/ml) exceeds the MICs of the low-level mupirocin resistant strains, so low-level mupirocin resistant strains can be treated by topical mupirocin19. On the contrary, high-level mupirocin resistant strains that can not be treated by mupirocin are more clinically important. Fortunately, low-level strains have so far been more frequently isolated than high-level strains. In our study, the prevalence of low-level mupirocin resistance (8.3%) was higher than the prevalence of high-level resistance (5.7%)2,10,20. However, high-level mupirocin resistant strains have been increasing in prevalence recently. Also, the mupirocin resistance rates were higher for the methicillin-resistant isolates than for the methicillin-susceptible isolates4,21. Chaves et al.21 detected a much higher percentage of mupirocin resistance among the isolates of MRSA (14.8%) than among the isolates of methicillin-susceptible S. aureus (0.6%). Therefore, the evaluation of mupirocin resistance, and especially high-level resistance, is very important in MRSA isolates.
High-level mupirocin resistant strains have an additional mupA gene in a plasmid that can be transferred to other strains by plasmid conjugation22,23. Bastos et al.23 showed that mupirocin resistance is transferred from mupirocin resistant strains of S. aureus to mupirocin susceptible S. aureus via a conjugative plasmid. Furthermore, this plasmid was transferred between S. aureus and Staphylococcus epidermidis. This result indicates the possibility of horizontal transfer of the conjugative plasmid among Staphylococcus species and this suggests that Staphylococcus epidermidis could be a reservoir of this plasmid. This enables the wide spread of mupirocin resistance. Further, the mupA gene may co-transfer with other antibacterial resistance, such as that against triclosan, tetracycline and trimethoprim3.
PFGE is the most widely used genotyping or genetic fingerprinting tool, although it requires technical skill, a long processing time and expensive instruments. It is commonly considered the gold standard method for epidemiologic typing and the determination of genetic relatedness11,24. Yoo et al.5 showed 20 of 25 high-level and 20 of 21 low-level mupirocin resistant S. aureus from eight long-term-care facilities belonged to the same PFGE groups. A study by Chaves et al.21 also identified that 13 of 14 high-level mupirocin resistant strains showed the same PFGE band patterns. These results indicate that clonal transmission of mupirocin-resistant S. aureus occurred in hospitals. In our study, 9 of 10 high-level mupirocin resistant MRSA isolates from (A) hospital and 5 of 6 low-level resistant isolates (2 from (A) hospital, 3 from (B) hospital) belonged to the same PFGE group.
The antimicrobial susceptibility of the mupirocin resistant strains can vary depending on different studies. A study conducted on 4980 MRSA strains showed mupirocin-resistant strains were more likely to be resistant to fusidic acid and to be susceptible to tetracycline, trimethoprim-sulfamethoxazole and ciprofloxacin as compared to that of the mupirocin-susceptible strains2. Yoo et al.5 showed all the mupirocin resistant S. aureus were resistant to oxacillin, penicillin and erythromycin and they were susceptible to ampicillin and vancomycin. In our study, the mupirocin resistant MRSA isolates were susceptible to vancomycin and rifampin, and they were resistant to ciprofloxacin, clindamycin and tetracycline. Compared to the low-level mupirocin resistant strains, the high-level mupirocin resistant strains were more resistant to erythromycin and fusidic acid.
Several agents have been shown to have activity against mupirocin resistant S. aureus3. These include azelaic acid, nitrofurazone and silver sulphadiazine. Maple et al.25 showed that the concentrations of azelaic acid, nitrofurazone and silver sulphadiazine close to the MIC were bactericidal, but mupirocin was only bactericidal at concentrations substantially greater than the MIC.
Prolonged use and frequent usage of mupirocin appear to be the most important factors for increasing mupirocin resistance. Riley et al.26 recommended less than 10 days treatment and at least 1 month between treatment.
The increasing number of reports of high-level mupirocin resistance could mean the potential loss of one of the major treatment methods for controlling MRSA. Therefore, mupirocin treatment should be used cautiously and judiciously. Careful monitoring of mupirocin usage and testing of S. aureus, including MRSA, for mupirocin resistance seems to be indicated.




 XML Download
XML Download