

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Medically, alopecia is viewed as a relatively mild dermatological condition. However, those suffering from the condition feel that alopecia is a serious condition with major distress on life and how other people view them1. As hair is an important component of identity and self-image, patients with androgenetic alopecia (AGA) may experience a distorted body image and negative feelings of social disadvantages2-6. Notably, even clinically imperceptible hair loss has been correlated with a decreased quality of life (QoL)7,8. Furthermore, Reid et al.7 demonstrated that patients may rate their hair loss as more severe than dermatologists. Consequently, understanding the psychosocial concern and QoL of patients with AGA has become a matter of great concern.
The aim of this study was to investigate the clinical and previous treatment factors, such as previous non-medical hair care experiences, reasons for hospital visits, age, duration, and severity of AGA, which can affect the QoL of AGA patients.
MATERIALS AND METHODS
Patients
In total, 998 male patients over the age of eighteen years were enrolled in the study from the dermatology departments of thirteen university hospitals in South Korea. Participants in this study were diagnosed with AGA by two independent dermatologists between March and April 2009. They included patients who visited a hospital for the treatment of alopecia and who visited a hospital for the treatment of other diseases, but showed clinical hair loss, which was sufficient enough to diagnose with alopecia. All patients were mentally and physically healthy. Patients with severe seborrheic dermatitis, alopecic disease, except for androgenic alopecia, and scalp disorders, such as scalp psoriasis and infection were excluded. Patients taking specific drugs, which can cause alopecia, such as corticosteroids, vascular dilators, antihypertensives, anticonvulsants, β-receptor blockers, bronchodilators, diuretics, spironolactone, cimetidine, diazoxide, cyclosporine and ketoconazole, over the previous 6 months, were also excluded. All patients provided written informed consent before participation, and this study was approved by the ethics committee of the Korean Hair Research Society.
Measures
1) Assessment of clinical characteristics
Patients were instructed to answer questions, such as previous experience in non-medical hair care and satisfaction ratings for the care, reasons for hospital visits, age, duration, and severity of AGA. Non-medical hair care includes hair cosmetics, shampoo, dietary therapy, hair massage and herbal therapy. Patients rated the satisfaction of non-medical hair care (10-point scale, where 0=ineffective result and 10=very effective). The reasons for hospital visits were divided into two categories, as treatment for alopecia and treatment for other skin diseases. To investigate the relationship between age and patient's QoL, the patients were separated into three groups: a group aged less than 30 years old, a group aged between 30 and 50 years old, and a group aged over 50 years old. The duration of AGA was separated into three groups: less than one year of alopecia, 1 to 5 years of alopecia, and exceeding 5 years of alopecia. Two board-certified dermatologists completed a severity of AGA questionnaire and rated the severity (2-point scale, where 1=mild and 2=severe) of patients with both clinically apparent and clinically imperceptible hair loss. Severity of AGA was assessed using a basic and specific (BSAP) classification. It was classified as either 'mild' or 'severe'9. BASP scale M1, M2, C1, V1, and F1 were recorded as 'mild', and BASP scale M3, C2, C3, U1, U2, U3, V2, V3, F2, and F3 were recorded as 'severe'.
2) Assessment of the QoL using the Hair-Specific Skindex-29
The Skindex-29 scale, which was originally developed by Chren et al.10, was modified to assess the QoL of patients with AGA. The words 'skin' and 'skin condition' on the Skindex-29 were changed to 'scalp' or 'AGA', respectively, and the Skindex-29 itself was renamed as the Hair Specific Skindex-29 (Table 1). This questionnaire consisted of three kinds of scales: a symptom scale (7 items), a function scale (12 items), and an emotion scale (10 items). Patients answered each question with a number ranging from 0 (never bothered) to 5 (always bothered). Answers to each item were transformed to a linear scale, ranging from 0 (never bothered) to 100 (always bothered). A scale score was the average score from the responded items and a global score was the mean of the sums of each scale. A high score indicates severely impaired QoL, and a low score reflects mild damage in the QoL.
Statistical analysis
To evaluate the correlation between clinical aspects and previous treatment history, and QoL, two methods were used for statistical analysis. First, the Wilcoxon Rank Sum test was used to analyse the clinical parameters, including the previous experience in non-medical hair care, reasons for hospital visits and severity of AGA affecting the value of hair-specific Skindex-29. Secondly, a Kruskal Wallis test was used to examine the effect of age and duration of AGA, which were classified into three groups on QoL of AGA patients. Multiple linear regression analyses were conducted to determine the statistical predictors of QoL, controlling for demographics and disease factors. Stata version 10.1 (StataCorp LP, College Station, TX, USA) was used for all statistical analyses and only p-values less than 0.05 were considered statistically significant.
RESULTS
Clinical characteristics of patients with AGA
Among the 998 patients, 138 patients (13.8%) experienced previous non-medical hair care. Non-medical hair care included hair cosmetics (57.2%), shampoo (15%), dietary therapy (14.8%), hair massage (7.2%) and herbal therapy (2.1%). Seventy four patients (54%) were dissatisfied, and 17 patients were satisfied with the non-medical hair care methods used. The causes for low satisfaction include a low effect (below expectations) (63%), high costs (22.2%), and a requirement of long-term treatment (13.6%). Four hundred and thirty two of the enrolled patients (43.3%) visited the hospital to treat their alopecia. The mean age of patients with AGA was 41.7 years (standard deviation [SD]±5.5). Six hundred of the enrolled patients (60.1%) had a mild severity score, and 398 patients (39.9%) had a severe severity score (Table 2).
Hair Specific Skindex-29 scores in patients with AGA
The mean global Hair Specific Skindex-29 score of the AGA patients was 27.3 (SD±19.1). The symptom scale score was 26.3 (SD±19.5), the function scale score was 24.0 (SD±20.1) and emotion scale score was 32.1 (SD±21.8).
Relationship between clinical profiles and QoL using Hair Specific Skindex-29
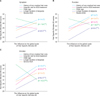
The QoL of patients with AGA was analyzed using several factors, including previous experience in non-medical hair care, reasons for hospital visits, age, duration, and the severity of AGA. Patients who had experienced previous non-medical hair care had higher Skindex scores on the symptom, function and emotion scales (p<0.05). Patients who visited the hospital for AGA treatment had higher scores on the function and emotion scales (p<0.05). The group aged under 30 had higher scores on all scales (p<0.01). The group with longer durations of AGA were more bothered and had a poor QoL (p<0.001). Also, the severe group had higher scores on all scales (p<0.05) (Table 3, Fig. 1).
The function and emotion scales of Hair Specific Skindex-29 correlated with all the clinical profiles, including previous experience in non-medical hair care, hospital visits to treat AGA, younger age, a longer duration of AGA and a severe AGA (p<0.05). The symptom scale correlated with only the previous experience in non-medical hair care, younger age and a longer duration of AGA (p<0.05) (Table 4, Fig. 2).
The global Hair Specific Skindex-29 significantly correlated with all those profiles.
Of special note, patients with a longer duration of AGA showed a prominent increase in the global score. (p<0.001) (Table 4). As shown in Fig. 3, QoL was poor in patients below the age of 30, and it was improved in patients between the ages of 31 and 50. However, QoL showed a decrease in patients over the age of 50, and this implies that the older the patient's age, the longer the duration of AGA and the greater the accumulated psychosocial distress.
DISCUSSION
Patients with AGA are significantly affected with self-image satisfaction, with potentially adverse psychosocial factors and with negative impact on a patient's QoL11. Alopecia has many known psychosocial complications, including depression, low self-esteem, an altered self-image, and less frequent social engagement7,11. Therefore, it has been suggested that physicians should address these psychosocial and QoL issues when treating patients with alopecia12. Although the Hairdex index was designed by Fischer et al.13, it is in limited use and is hard to utilize when comparing QoL of alopecia patients with patients that have other skin diseases. Therefore, we modified some terminology of the Skindex-29 to 'alopecia' or 'scalp', and then renamed it as the Hair Specific Skindex-29. For atopic dermatitis, psoriasis and acne, the Skindex scale is a validated, reliable, sensitive, and specific measure of how bothered patients are by their dermatologic conditions14.
However, a Skindex score has not been validated for use in AGA. Despite the widely reported psychosocial consequences of alopecia, each researcher used different kinds of tools, such as the Skindex-16, the Skindex-29, and the Dermatology Life Quality index and the brief COPE. Among those tools, the Skindex scale was recently used to measure the QoL of patients with hair loss7. Reid et al.7 demonstrated a relationship between hair loss and QoL, using the Skindex protocol. Also, the terms 'skin' and 'skin condition', used on the Skindex-29 scale, seemed to be confusing to patients who showed hair loss only on the scalp. Therefore, we suggest and hope that the Hair Specific Skindex-29 is used as a variant tool of the Skindex-29, and to be used to evaluate the QoL of patients with alopecia.
According to Kim et al.15, Korean patients with AGA receive incorrect information on the alopecia treatment. Furthermore, 60.9 percent of them use inappropriate, non-medical hair care products, and rarely get satisfaction; the current study was consistent with the previous findings16. AGA may have a marked psychosocial impact, in which the patients may seek inappropriate and unproven therapies that are available in nonmedical settings, often at great expense to the consumer17. Therefore, it is necessary to provide patients with correct information that is medically approved.
In regards to QoL in patients with AGA, experience in previous non-medical hair care, hospital visits for AGA treatment, young age, longer duration of AGA, and severe AGA were determined to be strongly correlated with poorer QoL. Patients with previous experiences in nonmedical hair care and hospital visits for AGA treatment tend to perceive their hair loss as worse. Furthermore, these findings demonstrate that patients' QoL are strongly and reliably correlated with the patient's perception of AGA. These results are in accordance with the findings by Cash16 in that persons seeking AGA treatment experienced more psychosocial impairment and substantial distress than the male controls.
Not surprisingly, patients of younger age and longer durations of AGA had a decreased QoL. Physical appearance is extremely important to most young men, and early onset of hair loss can have a definite negative effect on self-image and self-esteem. Low self-esteem makes life difficult when finding life partners and employment18. This result suggests that a longer duration of AGA may result in more severe hair loss, but tolerance of alopecia does not occur.
In conclusion, the strong relation found between patients' perception about their condition and the severity of AGA and patients' QoL in the current study suggests that patients with AGA have significantly decreased QoL. However, few studies have investigated therapeutic or supportive treatments that might improve their QoL. It is important that physicians consider the psychosocial impact of AGA on diverse areas of patient's lives. Physicians need to offer relevant treatment not just for hair loss, but for their emotional distress to AGA and functional consequences on their everyday lives. Our findings have implications for the treatment of patients diagnosed with AGA. Upon initial visit, the Hair Specific Skindex-29 questionnaire was given to each patient. Patients, with a low score of QoL were medically treated, but patients with higher scores of QoL might need both medical treatment and psychotherapy, as well. Further research is needed to better understand the effects of AGA and to improve treatment on self-image, psychological functioning and QoL.






 XML Download
XML Download