

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hand, foot, and mouth disease (HFMD), a common viral infection in childhood, is caused by enteroviruses, which are members of the Picornavirus family and most often associated with coxsackievirus A16 or enterovirus 71 (EV71)1,2. The disease derives its name from the characteristic papular or vesicular lesions involving primarily the skin of the hands, feet, and buccal mucosa3. In the majority of instances, HFMD typically follows a benign and self-limiting course. However, over the last decade this disease has emerged as a growing worldwide public health problem because of more frequent outbreaks with serious complications including neurological involvement, myocarditis, and pulmonary edema4-6. In the present report, we describe an unusual case of HFMD in combination with paroxysmal supraventricular tachycardia (PSVT) in an 11-month-old male infant. His parents consented to publication of this report and the accompanying photographs.
CASE REPORT
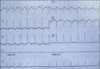
An 11-month-old male infant was admitted to the Department of Pediatrics, at the First Affiliated Hospital of Anhui Medical University in July 2010 with fever, fussiness, poor feeding, vomiting, and tachypnea over the previous two days. The birth and past medical history were nonsignificant, and the family had no history of similar disorders. Physical examination revealed the presence of sporadic papules and vesicles on his hands, feet, face, and perianal mucosa (Fig. 1). EV71 was identified from both throat swab and vesicle fluid by virus isolation techniques. An electrocardiogram revealed the patient's heart rate to be fluctuating in a very narrow range from 180~210/beats/min regardless of his physiologic state. P-waves were buried within or occurred just after regular, narrow QRS complexes (Fig. 2). Serum electrolytes and myocardial enzymes were normal. A chest x-ray and echocardiogram demonstrated no pathologic findings. The patient was diagnosed as having HFMD in combination with PSVT, based on the results of the physical examination, virus isolation, and electrocardiogram results. The child subsequently recovered well with symptomatic treatment, including intravenous administration of acyclovir, glucocorticoids, immunoglobulin, adenosine, and sotalol.
DISCUSSION
Our case had the distinctive features of typical skin lesions associated with HFMD in combination with PSVT. Determination of the etiologic agent, EV71, relied on laboratory identification. The combination of throat swab plus vesicle fluid was most useful, increasing isolation rates from 49% with throat swab alone, and 48% with vesicle fluid alone, to 67%7. EV71 is related to more serious complications8.
The risk factors contributing to severe HFMD are young male children (≤2 years old), atypical physical findings (tachycardia, tachypnea, hypotension, hypertension, bleeding in the gastrointestinal tract, and neurological deficits), a raised total leukocyte count, vomiting, and the absence of oral lesions9. Therefore, our patient was classified as a severe case due to the existence of several risk factors, including the fact that he was an 11-month-old male, with tachypnea, vomiting, the absence of oral lesions, and PSVT.
The precipitating factors of PSVT are often difficult to identify, but occasionally a febrile illness may give rise to an episode. Symptoms of PSVT in infants are inconspicuous and include irritability, poor feeding, tachypnea, diaphoresis, and poor color10. In the present case, the chief complaints were fever, fussiness, poor feeding, vomiting, and tachypnea, which might be attributed, in part, to PSVT. The mechanisms underlying the pathogenesis of PSVT caused by EV71 infection are unknown. However, in reference to PSVT associated with respiratory syncytial virus infection11-13, the following hypotheses may be relevant to understanding EV71 arrhythmia syndrome. EV71 first directly invades myocardial cells14; subsequently, lymphocytic infiltration, interstitial edema, and myocardial necrosis are triggered15; and associated postinfectious immunological reactions may persist for several months16.
The prognosis for HFMD is satisfactory. According to the latest report from Fuyang City, Anhui province, the fatality rate was only 0.4%17. Our patient also recovered well following the above-mentioned comprehensive treatments. PSVT was terminated within 36 hours of hospitalization and the lesions on his hands, feet, face, and perianal mucosa became crusted on the third day and proceeded to heal spontaneously.

 XML Download
XML Download