

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Fixed drug eruption (FDE) usually appears as bright or dusky red macules that may evolve into edematous plaques. FDE can develop from 30 minutes to several days after ingestion of medication1. On re-challenge, the skin lesion occurred again on the same location. This is the reason why it has been called "fixed" drug eruption2. FDE is most commonly associated with ibuprofen, sulfonamides, naproxen, barbiturates, and tetracyclines1. In addition, due to increasingly widespread use of imaging diagnosis, FDE has recently been observed after administration of contrast medium according to the frequency of use of organic iodine contrast media3,4. We present an interesting case of recurrent FDE diagnosed after administration of iopromide despite negative results in patch testing.
CASE REPORT
A 69-year-old male patient suffering from non-ST-elevation myocardial infarction was referred to our department on May 14, 2005. He developed several painful, annular, erythematous patches on both palms and trunk several days after receiving iopromide (Ultravist®, Shering, Berlin, Germany) for percutaneous transluminal angioplasty (PTA). He had undergone PTA four times using iopromide (Ultravist®, Shering, Berlin, Germany) from October 10, 2003 to May 13, 2005 and showed no adverse effect of the skin until then. A FDE due to iopromide was suspected clinically. The skin lesion was treated with topical methylprednisolone and desoxymethasone and showed complete resolution. One month later, we conducted a patch test with iopromide (as is, 1/3, 1/5, 1/10, and 1/100 in 0.9% normal saline) and control (0.9% normal saline) on the lesion and normal skin. However, results of the patch test with iopromide on both sites were negative at 48 hours and 96 hours. On November 26, 2008, the patient was mistakenly administered iopromide again. On the following morning, painful, reddish papules, and patches admixed with vesicles recurred on the same sites as the previous episodes, as well as on the genitalia (Fig. 1). For treatment, topical clobetasol propionate and methylprednisolone were applied for two weeks until the skin lesion completely disappeared, leaving pigmentation. Afterward, the patient was administered iopromide once again and similar skin lesions appeared on the same areas and also on the left arm, buttock, and leg (Fig. 2). The skin lesions resolved after application of topical steroids. We advised him to avoid taking iopromide in the future.
DISCUSSION
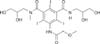
All intravascular contrast media are tri-iodinated benzene derivatives with iodine atoms in positions 2, 4, and 6. The other side chains give the contrast medium high water solubility and low toxicity. There are currently four types of products, ionic monomers, ionic dimers, non-ionic monomers (NIM), and non-ionic dimers. Most newer generation products are of the NIM type, including iopromide (Ultravist®, Shering, Berlin, Germany), iopamidol (Iopamiro®, Bracco spa, Milano, Italy), iomeprol (Iomeron®, Bracco spa, Milano, Italy), and iohexol (Omnipaque™, GE Healthcare, USA) (Fig. 3)3. Incidence of serious adverse reactions, such as anaphylaxis with the use of non-ionic contrast media (NICM), is lower than that with conventional ionic media, because NICM are not ionized in blood and exhibit lower osmolarity, compared to ionic contrast media. On the contrary, the frequency of drug eruption caused by NICM is higher than that with ionic contrast media4.
FDE typically has a late onset; therefore, it belongs to the category of delayed adverse contrast media induced reactions2. The majority of late skin reactions after contrast media ingestion are probably T cell-mediated allergic reactions5. Memory T cells are probably not circulating and remain only at the lesion, over the residual hyperpigmentation. This is the reason why the skin lesion occurs again on the same location and why it is so important that patch testing was performed on the lesion. Late reactions to contrast media have been shown to occur more frequently (8%) than immediate reactions (4%)6. The frequency of late adverse reactions to NIM has been reported to be between 0.52~23%5. To the best of our knowledge, there have been only three reports of FDE caused by NIM; iopromide2, iomeprol4, and iopamidol7 in the English literature. Two cases have documented positive reactions to iomeprol4 and iopamidol7 on the patch test. However, in another case, the patch test could not induce a positive reaction to iopromide2, as in our case.
Unfortunately, we observed a negative patch test with iopromide. The clinical information we obtained from the negative results is less clear since it has recently been shown that negative results are of low predictive value2. The negative patch test results might be attributed to the reagent preparation, vehicle used, inadequate transepidermal transepidermal absorption, and testing for the responsible agent outside of the lesional area. Although the patch test was negative in our case, we could confirm the diagnosis of FDE due to iopromide because the skin lesion occurred again at the same area after re-exposure to the same drug.
In addition, some cases have suggested the possibility of cross-sensitization among NICMs of similar structure2,6. Therefore, dermatologists and radiologists should keep in mind that NICM, such as iopromide, can cause FDE, and avoidance of the causative agent is the most useful method. In addition, patch testing with other contrast media should be performed for definite identification of both cross-sensitizing and non sensitizing contrast media2. We recommended that our patient undergo patch testing with other contrast media; however, he did not want further evaluation. Last, in order to prevent cutaneous reactions, patients who have previously undergone a series of FDE to contrast media are recommended to receive administration of intravenous injections of antihistamine and corticosteroid prior to future angiography5,6.


 XML Download
XML Download