

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Subungual squamous cell carcinoma is a rare condition. Its presentation can be deceiving; therefore, a high degree of vigilance is necessary in order to make an accurate diagnosis. Because other benign conditions can mimic the presence of malignancy, physicians must be able to identify such pathology in order to prevent delays in diagnosis1.
CASE REPORT
We report on a case of a 68 year-old healthy female who initially presented to the emergency room with pain, redness, and swelling in the regions surrounding the proximal and radial aspect of the nail fold of her right thumb in May of 2009. She noted that she had worsening symptoms over the course of one week but no prior history of similar events. The patient denied any trauma to the digit. She underwent an incision and drainage of what was diagnosed clinically as a paronychia. Cultures were positive for Staphylococcus aureus and she received IV antibiotics. The patient was discharged in stable condition with resolution of her symptoms.
She then presented four months later with pain along the radial aspect of her thumb with scant serous drainage from the lateral nail fold. She also pointed out the presence of a small amount of granulomatous tissue, which was subsequently resolved. She was followed conservatively and the drainage ceased. She continued to note occasional pain in the radial aspect of her nail fold as well as the interphalangeal joint. At this time, she was found to have what appeared to be a nail deformity (Fig. 1). The patient was taken to the operating room for a biopsy. The biopsy specimen was notable for moderately differentiated squamous cell carcinoma as well as pyogenic granuloma.
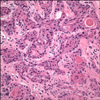
The cells showed nuclear pleomorphism, atypia, with increased abnormal mitoses and areas of keratin formation. The patient subsequently underwent re-excision of the nail bed, nail fold, and bone in the biopsy area with local flap reconstruction. Margins of the resection were measured 5 mm from the biopsy incision.
Two focal areas of squamous cell carcinoma were noted in the bony segment on final pathology (Fig. 2, 3, 4). The patient subsequently returned to the operating room for an amputation at the interphalangeal joint of the thumb. Due to the level of bony involvement, the patient underwent sentinel lymph node biopsy, which was negative for malignancy.
We employed the 7500 Real Time PCR system from Applied Biosystems for evaluation for the presence of human papillomavirus. DNA extracted from the specimen was probed for human papillomavirus (HPV) DNA isotypes 16 and 18. Neither HPV type 16 nor HPV type 18 was detected by Real time PCR. In order to further identify the presence of additional HPV isotypes, we utilized a qualitative in vitro diagnostic test for detection of fourteen high-risk HPV types through a pooled probe. The sample from total DNA extracted from tissue sections demonstrated a positive reaction only with HPV oligomix group 2, which includes oligonucleotides with target-specific affinity to HPV types 18, 39, 45, 59 and 68. Thus, at least one HPV isotype in our patient's specimen was positive.
DISCUSSION
Subungual squamous cell carcinoma is often thought to be an uncommon condition, which frequently leads to delay in diagnosis or misdiagnosis due to similarities in its presentation to other conditions, including pyogenic granuloma, paronychia, onychomycosis, keratoacanthoma, other tumors, warts, or trauma-related injuries2. With nail matrix involvement, the nail plate can become dystrophic, and, subsequently, result in onycholysis. This may perpetuate the onset of secondary infections.
Affected individuals are typically in the fifth through seventh decades of life. Digits of the hand are involved more often than those of the feet. Typically, one digit is involved; however, some studies have reported on simultaneous involvement of multiple digits3. The thumb, particularly the distal phalanx, tends to be the most commonly affected digit3,4.
Subungual squamous cell carcinoma seems to have a less aggressive course than those located elsewhere. According to reports in the literature, the duration of time from onset of a nail condition to diagnosis of squamous cell carcinoma varies greatly, from a few months to close to 35 years. Invasion of bone is found in approximately 20% of patients with subungual squamous cell carcinoma3. Metastasis and lymph node involvement is an atypical finding; however, it has been reported in a few cases.
Multiple predisposing factors, including chronic paronychia, HPV infection, radiation or sun exposure, trauma, and congenital ectodermal dysplasia, have been identified in the literature. Smokers may also have an increased predisposition5-7.
A strong association with HPV in relation to squamous cell carcinoma has been reported. Various research studies have identified a plausible transmission of HPV via genital-digital contact4. Multiple HPV types have been identified, including 16, 26 and 56 which have been shown to have associations with the presence of squamous cell carcinoma2,6. In one study, HPV DNA was identified by dot blot analysis of frozen tissue in 80% of patients with subungual squamous cell carcinoma. Of those, 60% demonstrated a relationship with the HPV 16 type4.
Proper biopsy of the nail bed is crucial for both diagnosis and future treatment options. A biopsy is prudent in all patients with chronic nail conditions that fail to respond to a reasonable trial of conventional treatment. To facilitate early diagnosis, recurrent nail infections or chronic ulcerations require a biopsy as well as cultures. Surgeons must carefully plan for future excisional needs should the lesion be malignant7. Careful removal of sufficient nail plate in order to provide adequate exposure is important. Incisional or excisional biopsy is usually followed by suturing of the lesion to an anatomic diagram of the affected area.
A rim of normal tissue should be included in the specimen. Acknowledgement of the depth and infringement of the lesion on adjacent tissue is critical. A proper discussion regarding the lesion and its orientation should be carried out between the surgeon and the pathologist7.
Treatment of squamous cell carcinoma is dependent on the extent of the tumor. With isolated nail bed involvement not extending to the periosteum, a wide local excision that usually involves nail fold, matrix, and nail bed removal to the periosteum is followed by a thinned full thickness skin graft7. Local flap reconstruction is also possible for superficial limited lesions. Recurrence rates are low (5%) with proper excision of the carcinoma8. On occasion, deeper infiltration may require partial bone excision en bloc with the tumor excision or even amputation at the distal phalangeal joint7. Due to the nature of the disease and frequent delays in diagnosis, bony invasion is believed to occur in approximately 20% of patients3,9,10.
While these tumors may be uncommon, practitioners must maintain high standards in promoting early detection and treatment. Adequate biopsy specimens can guide therapeutic measures for improvement of patient care7.



 XML Download
XML Download