

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Hidradenoma papilliferum is a benign, cystic, papillary tumor that originates from the apocrine gland or anogenital mammary gland; it occurs almost exclusively in the female anogenital area1-4. However, these tumors occasionally occur in a non-anogenital area and are referred to as "ectopic" hidradenoma papilliferum1,5-9. Ectopic hidradenoma papilliferum usually occurs in the head and neck region; most cases of ectopic hidradenoma papilliferum occur in the external ear or eyelid, where modified apocrine glands are found. Although ectopic apocrine glands are found normally in the nose, there has been only one case of ectopic hidradenoma papilliferum arising in nasal skin8. The tumor may show a variety of histopathological findings including cystic, tubular, papillary or solid pattern2-5. Herein we report a peculiar case of ectopic hidradenoma papilliferum on the nose.
CASE REPORT
A 43-year-old female complained of an asymptomatic tumor on her nose that had been slowly growing for 7 years. On physical examination, a 10-mm sized, pink-brown, elevated, firm nodule with a smooth surface was seen (Fig. 1).
The clinician's differential diagnosis included intradermal nevus, trichoepithelioma, and basal cell carcinoma. The tumor was excised and subjected to histopathological examination.
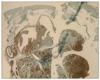
Microscopic examination showed a subcutaneous tumor that was well-circumscribed by connective tissue. Variously shaped cystic and tubular structures were seen. The lumina of those cystic structures were lined with a double or single layer of inner columnar and outer cuboidal cells. The cells of the lumina showed decapitation secretion similar to apocrine gland (Fig. 2). The epithelial cells of the lesion were strongly positive for gross cystic disease fluid protein (Fig. 3) and epithelial membrane antigen (EMA) (Fig. 4) but weakly positive for carcinoembryonic antigen (CEA) (Fig. 5) on immunoperoxidase examination. The lesion was excised, and the patient had no evidence of recurrence at 6-month follow-up.
DISCUSSION
Hidradenoma papilliferum is a benign adnexal tumor that mainly affects middle-aged women between the ages of 30 to 49 years (range, 25~66 years)10. It usually appears as a solitary, well-circumscribed, firm, flesh- to red-colored nodule of approximately 0.4 cm in diameter (range 0.1~1.0 cm)10. The nodule can also be umbilicated or cystic, and may be asymptomatic; however, bleeding, pain or pruritus can be associated1-4. Because these tumors occur almost exclusively in the vulva or perianal region, extragenital hidradenoma papilliferum are referred to as "ectopic hidradenoma papilliferum"9. Ectopic hidradenoma papilliferum has been reported in 19 people in the English dermatological literature5,6.
The clinical manifestations of ectopic hidradenoma papilliferum are similar to those of anogenital hidradenoma papilliferum. Lesions range in size from 0.5 to 6.0 cm; more than 85% of the lesions are about 1.5 cm in size9. The most common site of ectopic hidradenoma papilliferum is the head and neck region6-9. Lesions have occurred on the eyelid (3 lesions), forehead (2 lesions), face (site unspecified, 2 lesions), external auditory canal (1 lesion), postauricular area (1 lesion), scalp (1 lesion), and nose (1 lesion). Other lesion sites include the axilla, arm, thigh and back. Although the reason that most cases of hidradenoma papilliferum occur in the head and neck region has not been clarified, their location may be related to the distribution of apocrine glands. Apocrine glands are heavily concentrated in the anogenital area and axillae, most cases of hidradenoma papilliferum are located in the anogenital area. Modified apocrine glands are normally found in the external auditory ear canal, eyelid and breast. Thus the location of ectopic hidradenoma papilliferum corresponds to these common sites of apocrine glands and modified apocrine glands5-7. In our patient, it is possible that the heterotrophic apocrine gland normally found in the nasal skin may be related to the development of tumor. Therefore, the heterotrophic apocrine gland in the resection specimen may be heterotrophic apocrine glands adjacent to the tumor in the nasal skin8.
Histopathologic examination showed solitary, well-circumscribed, cystic spaces in the dermis surrounded by tissue with no connection to the overlying epidermis. Within the cystic spaces, multiple papillary projections into the cavity were seen. The lumen is usually lined with double or multiple rows of columnal cells or simple cuboidal cells with active "decapitation" secretion like that found in the apocrine gland. Although these invaginations that extend downward from epidermis and papillary projections can be found in syringocystadenoma papilliferum, the absence of connection in the papillary structure distinguishes hidradenoma papilliferum from syringocystadenoma papilliferum. Immunohistochemically, the hidradenoma papilliferum expresses EMA, CEA, gross cystic disease fluid protein (GCDFP)-15 and human milk fat globule membrane antigen (HMFG) and are usually positive for the markers of apocrine differentiation. Syringocystadenoma papilliferum usually express AE1/AE3, EMA and CEA, but the results of markers of apocrine differentiation including GCDFP-15 and HMFG are variable.
Although the exact pathogenesis of hidradenoma papilliferum is unclear, the fact that these tumors have only been reported after puberty suggests that estrogen receptor expression may be involved9. Regardless of the site and size, the treatment of choice is local excision and recurrence is unusual. Recently, some authors found similarities between hidradenoma papilliferum arising from extra-genital area and apocrine papillary cystadenoma11,12. The similarity of histopathology and apocrine differentiation in both tumors suggest that they may be identical tumors, but further study is needed.
The differential diagnosis includes syringocystadenoma papilliferum, tubular apocrine adenoma, and clear cell (apocrine) hidradenoma. Syringocystadenoma shows some cystic invaginations extending downward from the epidermis as well as plasma cell infiltration. In tubular apocrine adenoma, some dilated tubules with papillary projections extend into the lumen. In clear cell hidradenoma, the lesions are constructed with apocrine-like tubular structures and clear cells can be seen6.
The prognosis for hidradenoma papilliferum is good1-4. Malignant transformation of these tumors is rare and there are only 2 reports of carcinoma arising in a pre-existing hidradenoma papilliferum11.
In conclusion, we suggest hidradenoma papilliferum occurring on the nasal skin is a peculiar and interesting event.




 XML Download
XML Download