

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Syringocystadenoma papilliferum (SCAP) is a benign adnexal tumor, thought to arise from either pleuripotential appendageal cells or apo-eccrine glands1,2. It may occur de novo in children but frequently arises from a head or neck organoid nevus3. It is rarely found on the trunk or limbs and occasionally coexists with other tumors. Recently, SCAP associated with tubular apocrine adenoma (TAA) in the background of nevus sebaceous (NS) on the scalp and facial area has been reported2-10. However, the co-existence of these two tumors without background of NS on a non-scalp area has rarely been reported. Herein, we report an unusual case of SCAP associated with TAA on the calf area without pre-existing NS, which occurred de novo in an adult.
CASE REPORT
A 59-year-old male presented with a 10-year history of a leg nodule, which had increased in size recently. Physical examination revealed a 1.3×1.2 cm sized itchy, erythematous and lobulated nodule on the left calf. There were erythematous and slightly depressed crusted lesions on the surface area (Fig. 1). The lesion was completely excised. Upon microscopic examination, the superficial component was characterized by cystic invaginations of infundibular epithelium, lined by two layers of glandular epithelium (tall columnar luminar cells and cuboidal basaloid basal cells), with papillary projections. The glandular epithelium had areas of decapitation secretion (Fig. 2).
The epidermis overlying the tumor showed crateriform squamous cell lesions with mild nuclear atypia and focal dyskeratosis. Around this crateriform lesion, irregular invasion of the dermis by uneven, jagged, blunt ended epidermal cell masses and strands was observed (Fig. 3). Immunohistochemical stains taken for this lesion revealed all negatives for p53, p63, and Ki-67. The deeper portion had variable sized tubular structures, surrounded by increased collagenous stroma. The tubules usually contained two layers of epithelial cells; the outer layer had flattened cells, and the inner layer had columnar cells with decapitation secretion (Fig. 4). The findings in the upper level of the lesion were interpreted as SCAP and those in the deeper level were TAA.
DISCUSSION
SCAP has been reported to arise frequently in association with NS or basal cell epithelioma3. However, it occasionally coexists with other tumors originating from skin appendageal cells. In a study of 126 SCAP cases, Fujita and Kobayashi reported that SCAP was most frequently associated with sebaceous nevus (40 cases), followed by basal cell epithelioma (13 cases), sebaceous epithelioma (4 cases), apocrine hydrocystadenoma (4 cases), trichoepithelioma (2 cases), and eccrine spiroadenoma (1 case)11.
The association of SCAP with TAA was firstly reported in 1979 by Civatte et al.4. Since then, several similar cases have been described in the literature with common features of occurrence on the scalp and associated with NS4-10. Fisher12 described TAA as a minor variant of SCAP due to a clinicopathological similarity. However, Umbert and Winkelmann13 suggested that TAA is an independent clinical entity, consisting of a benign appendage tumor of apocrine origin, associated with organoid nevus.
TAA and SCAP may show histopathological overlaps, with some lesions having features of both neoplasms (SCAP+TAA). Kazakov et al.14 confirmed a morphological overlap between TAA and SCAP and demonstrateed a lack of universally accepted diagnostic criteria even among experienced dermatopathologists and pathologists. In this study, interobserver variability occurred when there were epidermal acanthosis, papillomatosis, and connections of neoplastic tubules to the overlying epidermis and/or follicular infundibula as well as plasma cell infiltration. These features accounted for the morphological overlap between TAA and SCAP.
Furthermore, SCAP is considered a hamartoma that recapitulates the formation of the folliculo-apocrine unit14. In this regard, TAA is interpreted as a deeper dermal tubular component of SCAP, rather than a combination of TAA with hamartoma15,16.
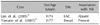
Cribier et al.2 reported that SCAP is the most common benign secondary tumor associated with NS. This is probably due to the presence of ectopic apocrine glands that are located in the deepest part of the NS, which can lead to either apocrine cysts or to SCAP. Thus, it is commonly located on the face and scalp. However, in our case there was no evidence of pre-existing NS upon microscopic examination. Only 2 cases of TAA associated with SCAP without NS of the scalp have been reported in the medical literature, and these cases are summarized in Table 1.
Our case demonstrates that SCAP with TAA can arise on non-scalp areas without a NS background in adults. Although the origin of SCAP and TAA and their relationships with follicular units need to be evaluated, we suggest that there can be SCAP lesions with TAA as a deeper component presenting on unusual sites.




 XML Download
XML Download