

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A cutaneous metaplastic synovial cyst (CMSC) is a rare cystic tumor in clinical dermatology. It is histologically characterized by a cystic cavity lined with metaplastic synovial tissue that is often hyperplastic and protrudes into the cyst's lumen as villous structures1. Further, CMSC is thought to develop in response to local trauma, and most reported cases have demonstrated a history of preceding trauma or postsurgical cutaneous scar1-8. The lesions clinically appear as erythematous and tender subcutaneous nodules, and are frequently misdiagnosed as suture granuloma.
Here, we report a case of CMSC in a 51-year-old female who presented with a cystic mass located on the left sole. She had no history of previous trauma or surgical procedures performed in the area.
CASE REPORT
A 51-year-old Korean woman presented with a 10-day history of a solitary, tender cystic mass on the left sole. She had no significant medical history, and upon physical examination, we found a solitary, relatively well-demarcated 3.0×3.0 cm-sized, skin-colored cystic mass on the left sole (Fig. 1). The patient experienced pain in the left sole whenever it touched the ground while walking. She denied any history of preceding trauma or any surgical procedure in that area. Serous fluid was discharged from the lesion as a result of aspiration.
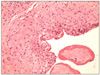
An incisional biopsy was performed at the lesion and included normal tissues. We observed a capsule-like fibrous layer and drainage of serous fluid. Histopathologically, there was no epithelial lining in the dermis; however, we observed a cystic structure with a large papillary projection that consisted of hyaline fibrous tissues (Fig. 2). The villous structures were lined by a membrane of varying cellularity, which mimicked the synovium. Some are composed of hyalinized connective tissue were covered with fibrin whereas others were highly cellular and were lined with multilayers of epithelioid and fibroblastic cells (Fig. 3). In some areas, the luminal cells were slightly flattened. Immunohistochemistry demonstrated that the cells lining the cyst were positive for vimentin, but negative for CD34 and CD68 (Fig. 4). Based on the histological findings, a diagnosis of CMSC was made.
We recommended excision to the patient to alleviate the discomfort experienced while walking, but the patient refused. We are currently monitoring her progress.
DISCUSSION
Since first described in 1987 by Gonzalez et al.1, 23 cases of CMSC have been reported in 12 English language studies1-12. The current CMSC case was rare as it was on the sole without a history of previous trauma or surgical procedure. Although the exact cause of CMSC has remained unclear, 13 of 23 reported cases have had histories of local trauma. Further, three of ten cases that have occurred spontaneously without local trauma were accompanied by Ehlers-Danlos syndrome3,10,12, which led us to believe that abnormal healing after microtrauma was a pathogenic mechanism of CMSC. Additionally, the fact that four cases of CMSC have accompanied rheumatoid arthritis6,9 and arthrosis10 suggested that chronic inflammation, constant pressure, and repeated manipulation have played critical roles in the pathogenesis of the lesions. Although the case presented in this report was a spontaneous case of CMSC that occurred without a history of trauma, it was believed to be caused by constant and chronic pressure since CMSC occurred in the first metatarsal head area, where heavy pressure was consistently applied.
CMSC lesions have been often misdiagnosed as suture granuloma given that the lesions are clinically associated with a surgical scar and observed as erythematous and painful subcutaneous nodules1,2,4,6,7. To this point, there have been two cases of multiple occurrences of CMSC6,11 and a single case of recurrent CMSC8.
Histopathologically, CMSC has been identified as a pseudocyst without an epithelial lining with a large papillary and villous projection observed along the center of the cavity inside the cyst. The thin layer that surrounds the papillation and cyst wall consists of cells that are very similar to the synovial membrane. The cyst wall is composed of various hypocellular and hypercellular areas. The hypocellular regions may appear somewhat hyalinized, and fibrin deposits may be seen in the cyst wall, while in the hypercellular area, one finds a mixture of epithelioid or spindle-shaped fibroblasts, mononuclear inflammatory cells, and sometimes multinucleate giant cells. Mitotic figures may also be seen in the cyst wall.
The lesion in the current case needed to be distinguished from bursitis. Bursitis has been observed as being histologically similar to CMSC in that the lining of the cyst is composed of a few layers of synovial or eosinophilic fibrinoid material. Bursitis shows fingerlike projections and is accompanied by fibrous connective tissue with infiltration of inflammatory cells13. In this case, the lesion was limited to the intradermal area and existed more superficially than observed with bursitis, as bursal sacs lie over bony prominences. Therefore, a diagnosis of CMSC was deemed to be more suitable.
From the perspective of immunohistochemical studies, the villous structures and lining reacted positively to mesenchymal intermediate filament vimentin and negatively to cytokeratin, allowing us to exclude that the CMSC lesions were of epithelial origin. Furthermore, studies reporting that S-100 and carcinoembryogenic antigen were stained negatively support the fact that the metaplastic synovial tissue was of mesenchymal origin1-8. The monocyte-macrophage lineage marker CD68 reacted negatively to the synovial lining and positively only in the histiocyte of the cyst wall. These findings were in contrast to CD68, which is typically manifested in a normal synovium. According to Bhawan et al.2, synovial metaplasia may not be of a synovial nature and may simply present an unusual reactive process induced by disruption of connective tissue. The fact that CD34, an endothelial cell marker, displayed negative findings substantiates that the cyst was not a variant of the vascular structure. The most effective treatment for CMSC has been surgery, and once cysts have been removed, there recurrence has been very rare10.
In conclusion, CMSC must be treated based on a differential diagnosis of a tender cutaneous cyst that occurs after a surgical procedure or a local injury. Specifically, this report demonstrated that CMSC should involve such a diagnosis s in instances of subcutaneous swelling in an area under constant pressure or stimulation, despite a lack of a history of specific trauma.



 XML Download
XML Download