

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Extraskeletal osteosarcoma (ESOS) is defined as a malignant mesenchymal neoplasm that produces osteoid, bone, and/or chondroid material, and is located in the soft tissues without attachment to the bone or periosteum1. ESOS occurs rarely, with an incidence of 4~5% of osteosarcoma2,3 and 1% of soft tissue sarcoma4. Up to 13% of cases have been reported with association to previous trauma or irradiation, but the etiological correlation of mechanical injury is difficult to assess1,5. It presents as a progressively enlarging soft tissue mass, which is painful in about one third of patients. The duration of symptoms vary from a few weeks to several months with a mean of 6.5 months4. Approximately 10% of reported ESOSs are superficially located in soft tissue. ESOS in skin develops de novo or by metastasis and is exceedingly rare. Herein, we describe a 56-year-old patient that presented with a nodule on a scar in the right girdle area, with a review of the literature.
CASE REPORT
A 56-year-old man presented with a painful, slowly growing nodule located on the right girdle area (Fig. 1). On physical examination, a firm, non-ulcerated, 1.5×0.8 cm sized, brown-colored exophytic nodule was observed on a linear scar of the right girdle area. The lesion presented 3 months ago, and had been preceded by intermittent pricking pain without specific skin lesions. Ten years ago, the patient went to a local physician with intermittent left foot pain. X-ray showed an osteolytic lesion in the fourth and fifth metatarsal bone of his left foot. He had undergone curettage and autogenous bone graft that was taken from the right iliac crest. Pathologic interpretation was osteoblastoma. He showed positive results for several weeks, but then developed pain and swelling on the distal portion of his left leg. X-ray showed progression of the osteolytic lesion and soft tissue swelling in his left foot. He had an additional biopsy for evaluation, which revealed osteosarcoma. Following that, an amputation was performed below the left knee. Postoperatively, he was not given adjuvant chemotherapy, radiotherapy or trauma in the tumor area.
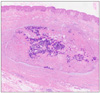
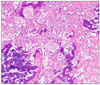
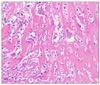
The tumor was excised with a clinical diagnosis of dermatofibroma. Microscopically, the tumor was confined to the dermis without connection to subcutaneous tissue (Fig. 2). Large amounts of thin and lace-like bony trabeculae and osteoid formed by neoplastic cells were observed in a highly pleomorphic sarcomatous stroma (Fig. 3). The neoplastic bone and osteoid exhibited an oteoblastic rim (Fig. 4). Immnunohistochemically, tumor cells were immunoreactive for vimentin, but negative for S-100 protein, desmin, and cytokeratin.
Beyond histopathological examination, physical findings and laboratory tests were within normal limits, and positron emission tomography-computed tomography (PET-CT) revealed no other bone involvement. The final diagnosis was primary cutaneous osteoblastic ESOS, which developed on previously traumatized skin as an operation scar. The patient improved without relapse or metastases for 18 months.
DISCUSSION
ESOS, initially described by Wilson6 in 1941, is a malignant mesenchymal neoplasm arising in soft tissues with no connection to skeletal structures, and composed of cells producing osteoid, bone, and/or chondroid material. Based on the predominant matrix, ESOS is divided microscopically into six distant subtypes, which include fibroblastic, osteoblastic, chondroblastic, osteoclastic or giant cell, telangiectatic, and small cell osteosarcoma1. ESOS usually occurs in patients over 40-years-old (mean age 47.5 years) with equal gender incidence; in contrast to primary osseous osteosarcoma its peak incidence in the 2nd decade of life. ESOS most commonly affects lower extremities, and in particular the thighs and other sites include the upper extremities, shoulder and retroperitoneum. A majority of cases of ESOS have been found in deep soft tissue7, but have rarely been confined to the subcutis or even the dermis2,5,8. The clinical course of ESOS is aggressive, and tumor- related mortality is 75% within 5 years of diagnosis. Tumor size (<5 cm versus ≥5 cm) appears to be the only reliable prognostic variable. However, histological subtypes are regarded by some as another variable of clinical course, and chondroblastic type has a slightly favorable outcome compared to the rest.
Cutaneous ESOS usually develops by de novo or metastasis. Skin as a primary site is rare and only 13 cases of primary cutaneous osteosarcoma have been reported to date (Table 1)5,7,9,10. With an exception of 2 undocumented cases, it occurred either on the cephalic area (5 cases) or in the extremities (lower leg 5 cases, and shoulder 1 case). The age distribution of primary cutaneous ESOS ranged from 51 to 96-years-old with a mean age of 70 years and most of them had a relatively short duration of less than one year. In most cases that occurred on the cephalic area, they arose at the site of a preceding insult, such as electrodessication (2 cases), radiotherapy (1 case) and trauma (1 case), whereas there was no previous insult in 6 cases that occurred in the extremities. Three cases that were over 5 cm in size were metastasized to the lung within a few months after initial diagnosis, but had no distinct histological types that were clearly related to the prognosis.
Bone tumor metastasis almost exclusively spreads hematogenously, and rarely by lymphatic dissemination, or direct dissemination to overlying skin of the primary lesion, or implantation11. A metastasis of bone tumor manifested by pulmonary involvement in the early stage and secondarily by involvement of other sites, such as distant bone, brain, lymph node, and other retroperitoneal sites12,13.
Cutaneous metastasis, whether from osteosarcoma or ESOS, appears to be exceedingly rare, as there are only 11 cases reported in the literature (Table 2)11-20. In most cases of skin metastasis, solitary or multiple lesions appeared, except in 2 undocumented cases, and all solitary lesions developed in the cephalic area.
The average age of metastatic cutaneous ESOS is 39.5 years lower than that of primary cutaneous ESOS, as it spreads to the skin from the osteosarcoma that is developed at an early age. Until cutaneous metastasis develops, they progress relatively fast at a mean of 12 months and are accompanied with distant metastasis to the lung or brain. It seems that there is no interrelationship between histological type and prognosis.
Due to the loss of data, we could not identify whether the histological type between the previous osseous osteosarcoma and the present cutaneous ESOS was identical or not. However, the previous tumor was completely removed and recurrence or other metastatic lesions were not observed. In addition, the interval of tumor development was quite long (10 years) compared to reported metastatic cases and no metastatic lesion on PET-CT was observed. Therefore, we diagnosed that this case was a primary cutaneous ESOS occurring on the operation scar. However, we could not completely rule out a metastatic ESOS because there was one report11, in which metastatic ESOS developed after 20 years of the primary osteosarcoma.
When making a differential diagnosis, bone forming soft tissue tumors such as myositis ossificans and sarcomas with osseous metaplasia including fibrosarcoma, malignant fibrous histocytoma, synovial sarcoma, epithelioid fibrosarcoma, and liposarcoma should be excluded. Other ossified tumors originating in the skin should also be considered. Osteoma cutis shows mature ossification without atypia or mitosis. Metaplastic ossification may also be seen in benign or malignant cutaneous tumors including pilomatricoma, intradermal nevus, desmoplastic malignant melanoma, basal cell carcinoma, and chondroid syringoma. In our case, the clinical and histopathological features supported a diagnosis of cutaneous ESOS.
Close long-term follow up will be needed for our patient including regular physical examinations and radiological studies because of less favorable osteoblastic histopathologic type, although the patient had a tumor less than 5 cm and no evidence of another distant metastasis was found, particularly in the lung.



 XML Download
XML Download