

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lichen planus pigmentosus (LPP)-inversus, a variant of LPP, is a rare disease that occurs mainly in the flexural areas1. Clinically it is characterized by the insidious onset of dark-pigmented macules and patches with or without pruritus. We now report a rare case of LPP-inversus in a 31-year-old woman. As far as we know, 17 cases have been reported in the world literature1-6.
CASE REPORT
A 31-year-old Korean woman presented with asymptomatic brown macules and patches of 5 years' duration located in the axillae, groin, and antecubital and popliteal fossae. The lesions initially began as a few small, asymptomatic macules clustered in the axilla, approximately 5 years prior to presentation. Over the last 2 years, the lesions increased in number and spread to affect the antecubital and popliteal fossae and groin. She denied any preceding erythema, pruritus, or vesicles before the appearance of hyperpigmentation. There was no previous history of medication use or trauma and no family history of pigmentary disorders.
On physical examination, there were multiple brownish macules and patches located in the intertriginous areas several millimeters to centimeters in diameter (Fig. 1). The larger lesions had a linear or annular configuration and the long axis of the linear lesions followed the lines of cleavage (Fig. 1A, B).
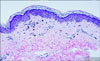
Biopsy of the macules in the antecubital fossae was done. Histologic examination revealed a regressive pattern of lichen planus with absent hyperkeratosis and hypergranulosis and a nearly atrophic epidermis. Hydropic degeneration of the epidermal basal layer was subtle but pigment incontinence was strongly expressed. The lymphocytic inflammatory infiltrate in the upper dermis was mild (Fig. 2).
Laboratory studies including a complete blood count, urinalysis, and liver and renal function tests were within normal limits.
DISCUSSION
LPP is an uncommon variant of chronic lichen planus that is characterized by hyperpigmented, dark-brown macules in sun-exposed areas and flexural folds that present both with and without pruritus. Kanwar et al.7 reported a study of 124 Indian patients with LPP wherein the face and neck were most commonly affected by hyperpigmentation. Flexural involvement including the axilla (8.9%), inframammary folds (6.5%), and groin (3.2%) was seen less frequently. Vega et al.8 published a clinicopathologic study of 11 cases of LPP describing distributions primarily in the face (73%) and trunk (45%). The axillary and inguinal folds were only affected in two patients. Several other studies have shown that the localization of LPP is typically not predominantly intertriginous9-11.
Pock et al.1 described seven central European Caucasians with LPP-inversus as a variant of LPP arising in intertriginous areas. The eruption of LPP-inversus occurs mainly in the flexural regions, including the axilla, infra-mammary, groin, popliteal and antecubital areas. Further, Kashima et al.3 recently reported two Japanese cases of LPP-inversus occurring in the axilla, groin, and popliteal fossae. The basic clinical and histologic data from reports of LPP-inversus are summarized in Table 11-6. Our case presented with asymptomatic brown macules and patches in the flexural areas showing a strong incontinence of pigment and a mild lymphocytic infiltrate in the upper dermis. Pock et al.1 proposed a possible morphogenesis of LPP-inversus wherein the lichenoid reaction occurs within a short period of time with dramatically intensive hydropic degeneration of basal keratinocytes. During this time, the compensatory increased proliferation of keratinocytes cannot develop as in typical lichen planus such that the papules transform quickly into brown macules. The predominant clinical lesion is macular and a histologic finding of intensive pigment incontinence is frequently identified. Our patient presented with chronic macular lesions that had been present for five years, which is likely why hydropic degeneration of the basal layer was subtle and the intensive lichenoid inflammatory reaction was absent.
The differential diagnosis includes ashy dermatosis and pigmented contact dermatitis. In the past, ashy dermatosis was thought to be the same condition as LPP. However, Vega et al.8 reported clinical differences between ashy dermatosis and LPP including the presence or absence of pruritis and lesion color. Pigmented contact dermatitis is a non-eczematous variant of contact dermatitis, characterized clinically by hyperpigmentation caused by common allergens such as fragrances, preservatives and deodorants. Our patient had no medication history and no reported contact of flexural areas with common allergens. The treatment of LPP-inversus is unknown. Some authors reported that the lesions gradually disappeared without medication within several months3. The paraneoplastic nature of LPP was described previously12. But there have been no reports of LPP-inversus associated with internal malignancy.
In conclusion, we have described a rare case of LPP-inversus in a Korean patient with diagnosis based on intertriginous location and histologic findings.


 XML Download
XML Download