

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acne scar and wrinkle are common cosmetic complaints1,2. Although various treatment modalities including botulinum toxins, dermabrasion, chemical peeling, and ablative or non-ablative laser skin resurfacing have been tried for managing these lesions, it is difficult to obtain satisfactory results when treated with only one method3-6. Therefore, to improve the success rate of treatment, it is important to understand the sequential histologic findings and skin surface characteristics following treatment.
Fractional photothermolysis is a treatment method that makes thousands of minute areas called microthermal treatment zones (MTZ) on the skin surface and transmits thermal injury to facilitate heat shock protein formation around the skin dermis, thus reforming collagen7. To date, a fractional photothermolysis system (FPS) based mainly on 1,550 nm erbium and 10,600 nm CO2 has been developed, and reported to be effective for the treatment of acne scars and wrinkles, with a shorter recovery period compared to traditional ablative laser.
Potential side effects after fractional photothermolysis include acneiform eruption, herpes simplex virus (HSV) outbreak, erosions, erythema, and post-inflammatory hyperpigmentation. To reduce these side effects for better outcomes, we need to understand the changes that occur in the skin of a patient after FPS therapy.
In this study, we investigated and compared skin surface characteristics after two kinds of fractional photothermolysis laser therapy with different wavelengths (1,550 nm, 10,600 nm) in Asian wrinkle and acne scar patients.
MATERIALS AND METHODS
Four patients (1 male and 3 females) with moderate to severe atrophic acne scars and another four (1 male and 3 females) with wrinkles were enrolled in this study. All the volunteers completed a total of three-months of follow-up. Each patient was observed prior to the treatment, as well as 1 day, 3 days, 1 week, 1 month, and 3 months after treatment (Fig. 1, 3). The age of the subjects ranged from 20 to 65 years (mean age: 40.75-years-old) and their Fitzpatrick skin types ranged from IV to V. The grade of acne scar and wrinkle in enrolled patients was evaluated by a qualitative grading system and a wrinkle severity rating scale8,9. The post-treatment condition of acne scars and wrinkles was evaluated using the following equipments: Sebumeter, Reviscometer, Tewameter, and Mexameter (MPA5®; Courage & Khazaka Electronic GmbH, Cologne, Germany). Following that, data analysis was performed using the Student's t test and statistical significance was defined as p<0.05. Written informed consent was obtained from each patient. Exclusion criteria included photosensitivity, pregnancy or lactation, history of hypertrophic or keloidal scarring, and use of oral isotretinoin or other physical acne treatments within the past 6 months. Patients with any medical illness that could influence the wound healing process were also excluded. Prior to each treatment, the face was cleansed with a mild, non-abrasive detergent and gauzes soaked in 70% isopropyl alcohol. A topical anesthetic cream (EMLA; AstraZeneca, Wilmington, DE, USA) was applied under an occlusive dressing for 30 minutes and subsequently washed off, after which regional nerve block was performed on the face. Eight patients with acne scars or wrinkles of the face were treated with two different wavelength FPS in their two symmetrical facial areas. On the right cheek of the patients, 1,550 nm erbium-doped fractional photothermolysis systems (Fraxel Xena®; Reliant Technologies Inc., San Diego, CA, USA) were delivered at a fluence/depth/coverage of 30 mJ/980 µm/20%. On the left cheek, 10,600 nm carbon dioxide fractional laser systems (Fraxel Repair®; Reliant Technologies Inc., San Diego, CA, USA) were delivered at a fluence/depth/coverage of 20 mJ/644µm/20%. Forced air-cooling was applied during the treatment to provide patients with comfort and compliance.
Therapeutic outcomes were assessed by standardized digital photography and patients' self-assessment of treatment outcome 3 months after treatment. Digital photographs of the face were obtained using identical camera settings (Olympus E-1; Olympus America, Inc., Melville, NY, USA) and lighting conditions at each follow-up session. The self-assessed level of improvement from the patients was evaluated using the following five-point scale: 0=no change; 1=slight improvement (0~25%); 2=moderate improvement (26~50%); 3=significant improvement (51~75%); 4=excellent improvement (>75%). In addition, all the volunteers were asked to report about pain during the laser treatment and make scoring with a 0-10 numeric pain intensity scale10,11.
RESULTS
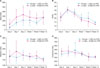
In patients with acne scars, 4 parameters associated with the healing process, such as sebum excretion rate, transepidermal water loss (TEWL), melanin and erythema index were evaluated. The degree of sebum excretion, measured using a Sebumeter, increased after treatment and then tended to slowly level off after 3 days. In addition, the magnitude of the increment was significantly higher on skin area treated with 10,600 nm FPS (p<0.01) (Fig. 2A). TEWL, which indirectly reflects skin barrier function, showed a rapid increase on day 1 post-treatment and then gradually decreased, eventually showing an overall decrease compared to the pre-treatment level (Fig. 2B). The melanin index increased on 10,600 nm FPS treatment area on day 1 post-treatment and showed a gradual decrease (Fig. 2C). The erythema index increased at day 1 on both skin areas, but increased at day 3 only on the skin area treated with 1,550 nm FPS (Fig. 2D).
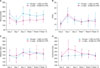
In patients with wrinkles, the Reviscometer that was used to measure elasticity of the skin, showed a decrease on day 1 post-treatment, subsequently exhibiting a sharp increase, and eventually recovering almost to the pretreatment level after 3 months on the skin area treated with 1,550 nm FPS (Fig. 4A). On the other hand, a decreased Reviscometer score was maintained for a longer period of time in the wrinkle area treated with 10,600 nm FPS. TEWL, as seen in patients with acne scars, increased at day 1 after treatment and then gradually decreased, eventually recovering almost to the pre-treatment level (Fig. 4B). The melanin index slightly increased starting on day 1 post-treatment but at 3 months after treatment, did not show a significant difference compared to the measurement before treatment (p>0.05) (Fig. 4C). The erythema index rapidly increased in the 10,600 nm FPS treatment area compared to the 1,550 nm FPS treatment area and then gradually decreased, eventually recovering to the pre-treatment level after three months (Fig. 4D).
The subjective satisfaction rating was evaluated three months after one session of treatment with each FPS, and both acne scar patients and wrinkle patients showed a slightly higher satisfaction rating in the 10,600 nm FPS treatment area (Table 1). In acne scar patients, the pain score was 5.5±2.7 when treated with 10,600 nm FPS, and 2.4±1.7 when treated with 1,550 nm FPS. On the other hand, in wrinkle patients, the values were 6.1±1.4 and 3.7±1.3, respectively. The intensity of pain during treatment was significantly higher in patients treated with 10,600 nm FPS (p<0.01, in the acne scar and wrinkle patients, respectively).
DISCUSSION
FPS is a product of MTZ theory. Traditional ablative type laser ablates the entire skin surface, leaving areas with less collagen formation due to lack of heat shock protein in the central area of treatment. It also has a long recovery period and renders the tissue vulnerable to infection at the site of treatment. The non-ablative type laser that was developed later, transmits energy to the dermis without damaging the skin surface and inducing collagen reformation, has reduced adverse effects of ablative type laser, but the effect is insufficient and short-lived. FPS, aimed to overcome the shortcomings of ablative and non-ablative type lasers, amplifies the effect of treatment and minimizes the recovery period by creating thousands of minute areas on the skin surface and transmitting thermal injury to facilitate heat shock protein formation around the skin dermis, thus reforming collagen. In other words, laser is irradiated as innumerable dots into a small area, resulting in a tiny wound in which tissue reaction is induced on the irradiated area, while the rest of the tissue remains intact, facilitating wound recovery. Therefore, a more natural recovery and shorter recovery period is possible.
Histologic finding after the application FPS showed that in the case of 1,550 nm Er-glass FPS, the epidermis regenerated by keratinocyte reformation and homogenization of dermal matrix, as well as the formation of microscopic epidermal necrotic debris12, whereas in the case of 10,600 nm CO2 FPS, healing was mainly achieved by an increase in substances related to wound healing such as heat shock protein, procollagen and dermal elastin around the coagulation column after formation of ablative microlesion13,14.
In this study, skin surface characteristics after treatment were measured by a non-invasive method. As a result, both types of FPS showed a significant increase in TEWL, implying that skin barrier damage had occurred, which gradually decreased after treatment and recovered almost to the pre-treatment level after 1 week. Because of this kind of skin barrier defect, infections such as HSV infection and folliculitis can increase15,16. To compensate this, an active application of dressing or skin regenerative agents and moisturizers is needed. As for the sebumeter in acne patients, sebum excretion increased more in the 10,600 nm treatment area, and is thought to be a factor in the occurrence of acne or folliculitis after treatment. Therefore, topical antibiotics or oral antibiotic medication may be needed, and post-treatment occlusive dressing or moisturizer should cautiously be applied. With the reviscometer that took measurements 3 months after treatment, the decrease in the score was more sustained in the 10,600 nm FPS treatment area compared to the 1,550 nm FPS, showing superior improvement with wrinkles, and patient satisfaction rating was higher in the 10,600 nm FPS treatment group. However, the numbers of the samples are too small to make a clear conclusion.
The disadvantages of FPS treatment include pain during irradiation, erythema, and pigmentation. As a result of this study, we found that the pain felt by patients was greater in the areas treated with 10,600 nm FPS. As for erythema and pigmentation, the erythema index and melanin index rapidly increased in the 10,600 nm FPS treatment area compared to the 1,550 nm FPS treatment area, but after 3 months both areas did not show any significant difference compared to before treatment, thereby proving both types of FPS to be a safe treatment.
This study is not without limitations. For ethical reasons and suggestions from the institutional review board, we did not perform a skin biopsy at the site of laser irradiation after laser therapy. Therefore, we were not able to obtain histopathologic data such as collagen and elastin. As a first preliminary study, the duration of follow-up for the treated patients was only 3 months in this study, but for recording of the possible later onset side-effects, it is better to prolong the duration of follow-ups. Complementary studies with post-treatment histological examinations and longer follow-ups are needed to validate our early findings.



 XML Download
XML Download