

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Varicella-zoster virus (VZV) is a highly contagious virus that causes varicella upon primary infection and remains latent in the sensory ganglia of spinal or cranial nerves. Throughout a person's life, newly-invading VZVs and those reactivated from the sensory ganglia continuously stimulate the immune system. However, herpes zoster (HZ) can occur with increasing age1,2.
As with other developed countries, Korea is becoming an aging society. Also, the prevalence of diseases that increase the risk of HZ, such as diabetes mellitus and hypertension, are increasing3,4. Moreover, the number of transplantation patients, in whom the immune response is suppressed for therapeutic reasons, is rising, which may further increase the number of HZ patients. The United States has recognized the increase of HZ due to the routine vaccination of children against varicella. Routine vaccination reduced wild type VZV, which in turn diminished the natural boosting effect in adults. Therefore, since 2008 it has been recommended that US adults ≥60-years-of-age be vaccinated for HZ5. Varicella vaccination has been included in the routine vaccination regimen of children in Korea since 2005. Drawing on the US experience, the expectation in Korea is for a decreased prevalence of wild type VZV. However, the reality is unclear since little is known regarding VZV immunity in Korean adults.
There are several methods to measure protective immunity against VZV. The fluorescent antibody to membrane antigen (FAMA) method best represents the neutralizing antibody titer, which shows protective immunity to varicella. However, various limitations of FAMA have prompted efforts to develop a glycoprotein enzyme immunoassay (gpEIA) method.
In this study, the gpEIA antibody titer and FAMA positive rates were measured to obtain data concerning protective immunity against VZV in Korean adults over 40 years of age. Also, we examined whether age, and/or previous HZ history affects the level of immunity.
MATERIALS AND METHODS
Subjects
Subjects were 214 healthy adults ≥40 years of age from Daegu city who were free of infectious disease or autoimmune disease. After informed consent was obtained from each study participant, each subject completed a survey and blood was collected. All procedures followed a protocol (PCR-09-23) approved by the Yeungnam University Medical Center's Institutional Review Board.
Measurement of gpEIA antibody titer
The measurement of gpEIA antibody titer utilized a VaccZyme™ VZV gpEIA kit (Binding Site, Birmingham, UK) following the manufacturer's instructions. An antibody titer <100 mIU/ml was interpreted as susceptible to infection, 100~150 mIU/ml as equivocal, and ≥150 mIU/ml as protective.
Fluorescent antibody to membrane antigen test
The MGLu human embryonic lung fibroblast cell line was generously provided by Mogam Biotechnology Institute (Yongin, Korea). Cells were cultured using Dulbecco's Modified Eagle's medium (Lonza, Basel, Switzerland), 10% fetal bovine serum (Lonza), 1% antibiotic-antimycotics (Gibco, Carlsbad, CA, USA) at 37℃ in a controlled atmosphere of 5% CO2. After 48 h incubation, cells were infected with Varilrix™ (GSK, Brentford, UK) and then incubated at 35℃ in an atmosphere of 5% CO2. When 60~70% of the cells displayed a cytopathic effect, cells were harvested with 0.05% Trypsin-EDTA (Gibco) and were used as the FAMA antigen. The FAMA method was done as described previously6. Anti-VZV antibody (National Institute for Biological Standards and Control, Potters Bar, UK) was used as a positive control. Serum with a gpEIA titer of 10 mIU/ml obtained from a child with no history of varicella and who had not been vaccinated was used as a negative control.
Statistical analysis
A linearity test using the χ2 test was done to verify whether increasing age strongly correlated with increasing antibody titer for VZV. In addition, for the change in the geometric mean titer (GMT) with age, an ANOVA test was used. The test compared the means of various groups and assessed the linearity of the change. A t-test was used to check if there was a difference between the averages of the two groups according to HZ history. All p-values were two-sided and were considered significant at <0.05.
RESULTS
Age, sex and HZ history of subjects
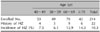
Of the 214 subjects, 53 were aged 40~49 years of age (average age 43.8 years), 49 were 50~59 (average age 54.7 years), 70 were 60~69 (average age 64.9 years) and 42 were ≥70 (average age 73.7 years) (Table 1). There were 91 males (42.5%) and 123 females (57.5%). Twenty-two of the 214 subjects had a HZ history: four of the 22 were aged 40~49 years, three were 50~59, nine were 60~69 and six were ≥70 (Table 1). This represented a HZ incidence rate of 10.3%, which was equivalent to 7.5% of those aged 40~49, 6.1% of those aged 50~59, 12.9% of those aged 60~69 and 14.3% of those aged over 70 (Table 1). The difference in HZ incidence rate among the different age groups was not significant because only a small number of subjects had a HZ history (cross tabulation, p=0.173).
gpEIA antibody titer level and distribution for respective age groups
One hundred ninety three subjects (90.2%) had a protective level against varicella (>150 mIU/ml), seven (3.3%) had an equivocal level of 100~150 mIU/ml, and 14 (6.5%) had a susceptible to infection level of <100 mIU/ml (Table 2). Among each age group, 86.8%, 87.8%, 91.4%, and 95.2% had a protective antibody titer in aged 40~49, 50~59, 60~69, and over 70, respectively. Again, there was no significant correlation with increasing in age (crosstabs, p=0.163) (Table 2). The gpEIA antibody titer range was 1.2~4.22 log10 mIU/ml (16~15,849 mIU/ml), and 38.8% of adults were in the range of 2.4~2.7 log10 mIU/ml (251~501 mIU/ml) (Fig. 1). From age 40 to 69, the distribution of the gpEIA titer showed a similar pattern, however, more subjects who were ≥70 years of age had over 3.2 log10 mIU/ml (1,585 mIU/ml) compared to the other age groups (Fig. 1).
Antibody titer distribution and gpEIA GMT depending on zoster history
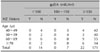
Among adults who did not have HZ, the gpEIA antibody titer was distributed as 171 (89.1%) in the protective level, 7 (3.6%) in equivocal, and 14 (7.3%) in susceptible to infection (Table 3). However, among those who previously had HZ, all were in the protective level (Table 3). The average gpEIA GMT of the 22 adults who previously had HZ was 1,122 mIU/ml, which was higher than the average gpEIA GMT of 457 mIU/ml of the adults who did not have a history of HZ (Table 4). The gpEIA GMT of all adults was 490 mIU/ml and increased with age. GMT was 417 in those aged 40~49, 437 in those aged 50~59 and 60~69, and 741 in those ≥70 years of age (Table 4) (ANOVA, p=0.02).
FAMA seropositive rate
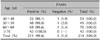
The FAMA seropositive rate for all adults was 98.6% at a serum dilution of 1:4 and the seronegative rate was 1.4%. The FAMA positive rate in those over 70 years of age was 100% (Table 5). There was no significant difference between age groups (χ2 test p=0.60). When FAMA was compared with the gpEIA antibody titer level, those who had protective level of gpEIA antibody titer were all FAMA positive (Table 6). In the equivocal range five of seven individuals were FAMA positive and two were negative. For those in the susceptible to infection level, 13 of 14 were FAMA positive and one was negative (Table 6).
DISCUSSION
Methods to measure VZV antibody titer are diverse, and different methods may be chosen depending on whether the object of the study is to diagnose previous infections or to measure the protective immunity for prevention of disease. The enzyme-linked immunosorbent assay (ELISA) is usually used to diagnose infection by varicella. However, neutralizing antibody plays an important role in preventing varicella. Therefore, in the early days of varicella vaccine development, the neutralizing antibody test or FAMA assay was used to measure vaccine induced immunity. However, these methods are not suitable for testing a large population, which has prompted the more recent use of the gpEIA method. This method exploits glycoprotein antigens that exist on the envelope of VZV. Because gpEIA can represent the neutralizing antibody titer, is easy to use, and can test a large population in a short period of time, it is currently considered as the most appropriate method for testing protective immunity against VZV. The problem in measuring VZV antibody titer is that different antibody titer units are used among ELISA kit manufacturing companies and methods, rendering it difficult to cross-compare. For this reason, an international standard of antibody titer for protective immunity has yet to be set. To address this problem, in 2006 fourteen European countries tried serologic standardization for VZV using five types of ELISA kits, immunofluorescence assay, complement fixation test and FAMA from 13 laboratories. As a result, when a diagnostic ELISA kit is considered, it is categorized as negative if the geometric mean antibody activity is <50 mIU/ml, equivocal if it is 50~100 mIU/ml, and positive if it is >100 mIU/ml7. However, there is little data for gpEIA antibody titer, as the technique is in an early stage of development. The gpEIA kit by Merck, Sharp & Dohme Research Laboratories, which has been used for the longest time in the US, is not commercially available and since it was invented to evaluate the immunogenicity of varicella vaccine, it is not suitable for measuring antibody titer in adults due to natural infection. Furthermore, it uses its own units, which makes it very hard to compare with other study results8,9. The VaccZyme™ gpEIA kit used in our study adopted a World Health Organization international standard VZV immunoglobulin as the antibody titer calibrator, so it can display the antibody titer in standardized international units. This makes it possible to compare our data with data for later studies. The antibody titer interpretation guideline was set based on British adults naturally infected by varicella, so it is suitable for measuring the antibody titer for adults.
Little is known of the seroprevalence of antibodies against VZV in Korean adults. According to a 1997 study where the subjects were hospital employees in their twenties to fifties and in which a Behring Enzygnost IgG kit was used, the average seropositive rate was 96.2%; 94.8% in those aged 20~29, 98.9% in those aged 30~39, and 100% in those aged 40~59. However, there were only nine subjects aged 40~49 and two subjects aged 50~5910. In the present study, considering a gpEIA antibody titer ≥150 mIU/ml as being indicative of protective immunity, the seropositive rate in all people over 40 was 90.2%; 86.8% for those aged 40~49, 87.8% for those aged 50~59, 91.4% for those aged 60~69, and 95.2% for those ≥70. This was lower than that measured using the Behring Enzygnost IgG kit, but the trend of increasing seropositive rate with increasing age was similar. The Behring Enzygnost IgG kit is a kit used for diagnosis of previous infections, and can detect antibodies against various structural proteins of VZV as well as nonstructural proteins, so it does not represent protective immunity. Its determining levels are ≥110 mIU/ml for positive, so its seropositive rate can be different from that measured using gpEIA.
The FAMA assay is a method developed by Williams et al.6 in 1974, which has very high sensitivity and specificity against antibody that reacts to glycoproteins of VZV. Hence, FAMA is regarded as the gold standard method for measuring protective antibody titer against varicella6. In our previous FAMA experiment done with sera from 138 children, 113 of the sera that had a gpEIA antibody titer over 50 mIU/ml were FAMA positive (unpublished data). So, we assumed that sera having a gpEIA antibody titer ≥150 mIU/ml (protective level according to the gpEIA kit guideline) were FAMA positive, and the FAMA assay was performed only for cases in which the antibody titer was <150 mIU/ml. The FAMA seropositive rate in all adults was 98.6%, and in those over 70 years of age was 100%, so most of the adults had antibody against VZV. The FAMA seropositive rate was a little higher than the seropositive rate of the gpEIA protective level, which was probably due to the high sensitivity of the FAMA method.
In this study, 10.3% of the 214 Korean adults over 40 years of age previously had HZ. A large scale cohort study in other countries showed the incidence rate of HZ to be 3.9~11.8% for people older than 60 years of age, so these results are similar to the incidence rate in our study1,11-15. The gpEIA GMT of adults who had not had HZ was 457 mIU/ml, while that of those who had HZ was higher at 1,122 mIU/ml. It was reported that cell-mediated immunity may alleviate the symptoms of HZ while antibody has no relation to alleviating the symptoms16,17. However, the present data suggest that those who had HZ have a meaningfully high gpEIA antibody titer, which implies that when HZ occurred, the reactivated virus stimulated humoral immunity. Currently, the US government recommends HZ vaccination for adults over 60 years of age, and development of the vaccine is underway in Korea as well. A US study also reported that the gpEIA antibody titer increases after 3 weeks of HZ, and HZ vaccine can induce not only cell-mediated immunity but also an increase in the gpEIA antibody titer 6 weeks after vaccination17,18. Therefore, while cell-mediated immunity is an important marker when evaluating the immunogenicity of HZ vaccine, gpEIA antibody titer may also be used as a biomarker for determining whether the immune system has been stimulated by the vaccine.




 XML Download
XML Download