

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Parry-Romberg syndrome (PRS), or progressive facial hemiatrophy, was first described by Parry1 in 1825 and Romberg2 in 1846. PRS is a rare disorder of unknown origin, usually developing in the first or second decade of life3,4. This condition is characterized by slowly progressive unilateral facial atrophy of the skin, soft tissue, muscles, and underlying bony structures. PRS commonly affects dermatomes of one or multiple branches of the trigeminal nerve5. Atrophy may be preceded by cutaneous discoloration of the affected skin, such as hyperpigmentation or depigmentation. Hairless patches may also be observed in the affected scalp6.
The incidence and etiology of PRS are still not well known because of its rarity. There is an age-old debate regarding the relationship between PRS and linear scleroderma since they possess similar clinicopathological appearances. Some assert that PRS and linear scleroderma are distinct, but frequently accompanying disorders7, while others include PRS in the same spectrum of linear scleroderma. Plastic surgery using large buried pedicle flaps of dermis and fat, or silicone implants offers some cosmetic benefits. However, the therapeutic modalities are limited and unsatisfactory.
Here, two uncommon cases of PRS accompanying en coup de sabre are described and a discussion of whether these conditions are closely related is provided.
MATERIALS AND METHODS
Case 1
A 37-year-old woman visited our department with a 7-year history of progressive atrophic change on the right side of her face. She first had noticed that areas superior to the right forehead and cheek were hypopigmented seven years ago, at which time she was diagnosed with vitiligo elsewhere. Four years later, atrophy and depression appeared on her nose. After the manifestation of atrophy on the right upper lip and gingiva, a fat graft was conducted. She was referred to our department for persisting brownish atrophic patches on the right cheek and forehead, as well as painful, dry lips. Close examination revealed an ivory-colored hard immovable patch on her forehead, and a soft non-adhesive brownish patch on the same side of the cheek. Moreover, sclerotic recession was observed on her right nasal alae, right upper lip and gingiva (Fig. 1).
There was no family history of similar lesions, nor specific personal trauma or medical history. Laboratory tests, including liver and kidney function tests, showed no remarkable findings, except for antinuclear antibody (ANA) showing a 1:80 positive in a homogenous pattern. Skeletal abnormalities were not found upon X-ray examination of the skull. Physical examination revealed no signs of neurologic abnormalities. The patient refused further radiological studies of the head including computed tomography (CT) or magnetic resonance imaging.
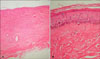
A skin biopsy taken from the right forehead showed an atrophic epidermis and a thickened dermis composed of abundant collagen bundles. There were few inflammatory cell infiltrations in the dermis (Fig. 2). The histologic findings were compatible with scleroderma. Based on the clinical and histological findings, the patient was diagnosed with PRS accompanied by unilateral en coup de sabre.
The patient was treated with topical steroid cream for her right upper lip and intralesional steroid injections for the indurative plaque on her right forehead. It was recommended that she be treated continuously, but she stopped the visits without any improvements.
Case 2
A 29-year-old woman presented to this hospital department with an 18-year history of gray atrophic patches on her right face. She first had gray atrophic patches on the right side of her chin and neck, and dark brownish sclerotic vertical plaque on both sides of her forehead (Fig. 3). On that occasion, depressions on the cutaneous surface were not distinctive. The lesion had been asymptomatic and not preceded by any trauma. A previously conducted skin biopsy of her forehead confirmed the diagnosis of localized scleroderma. Over the succeeding years, the sclerotic change and atrophy gradually spread to the right side of her nose, periorbital area, forehead, and scalp (Fig. 4A, B). The patient noticed the continuous recession of the lesions. Physical examination of bilateral linear streaks of the forehead revealed a sclerotic tan color extending longitudinally from the frontal scalp to the eyebrow (Fig. 4C, D). Her past treatments included the scapular osteocutaneous flap, mandibular maxilla distraction, and fat graft and injection.
In addition to a lack of trauma, the patient also had no specific previous medical history or related instances in her family history. The results of laboratory studies, including liver and renal function analyses, were within normal limits, and various serologic autoantibodies were negative. Radiographic evaluations using X-rays including panoramic radiography of the teeth and brain CT revealed no abnormal findings.
After diagnosis of PRS with bilateral en coup de sabre based on the clinicopathologic findings, we administered oral penicillamine. However, the patient declined prolonged treatment because of an incessant headache. Therefore, the patient was subsequently treated with intralesional injections of steroid into indurative plaques on both sides of the forehead and scalp, but the lesions persisted. Because the clinical results were unsatisfactory, she was referred to the department of plastic surgery for the further surgical corrections.
DISCUSSION
PRS is an uncommon degenerative condition characterized by a slowly progressive atrophy that is generally unilateral, and impacts facial tissue, including muscles, bones and skin. The incidence and cause of these alterations are unknown5,8. A cerebral disturbance of fat metabolism has been proposed as a primary cause9,10. Trauma, viral infection, endocrine disturbance, autoimmunity and hereditary are also believed to be associated to the pathogenesis of the disease11-15. However, there was no history of trauma, infection, or underlying autoimmunity in the present cases. The onset of this syndrome often occurs during the first and second decades of life, after which the atrophy slowly progresses over several years, eventually becoming stable11,16-18. However, some patients may have a reactivation of inactive lesions, and the final degree of deformity is usually dependent on the duration of the disease17.
Treatment is still unsatisfactory and limited. Many have attempted to transfer autologous fat tissue to atrophied lesions18. Injection of silicon, bovine collagen and inorganic implants are considered as useful alternatives18,19. However, cosmetic revision is not recommended until the progression of the illness is complete5. Nevertheless, these methods do not completely restore the former appearances because the structures become extinct with time owing to gravity and the absorption of implanted materials. In the current cases, surgical corrections and intralesional steroid injections had been performed, but the patients were not satisfied with the outcome, and we are still searching for new effective modalities.
Many studies have suggested that a close relationship exists between PRS and linear scleroderma, especially en coup de sabre. There have been confused assertions considering the relationship between PRS and en coup de sabre in previous reports because the clinical presentation of en coup de sabre may appear similar to PRS. Moreover, the frequent reports of the coexistence of both diseases may make them much difficult to distinguish. En coup de sabre morphea refers to a lesion of linear morphea that is generally unilateral, and extending longitudinally from the forehead into the frontal scalp20. Paramedian locations are more common than median placements. The involved skin area is depressed, hard, hyperpigmented, and shiny, and may accompany hairless patches.
Many discussions of the relationship between PRS and en coup de sabre eventually condense into two considerations, two distinct disorders, or a continuum. Orozco-Covarrubias et al.7 regarded these two diseases as separate entities because there are differences between PRS and en coup de sabre with respect to their cutaneous and histopathological features. Even though both are rather similar, they thought that the cutaneous sclerosis, hyperpigmentation, and alopecia usually developed in en coup de sabre, while PRS does not show cutaneous sclerosis at any stage. Conversely, Blaszcyk and Jablonska21 described the conversion of en coup de sabre into PRS and suggested that PRS may be a deep variant of en coup de sabre based on the observation of en coup de sabre existing before the development of PRS. Recently, Tollefson and Witman22 also supported the previous belief that both diseases are on the same spectrum. The prevalence of en coup de sabre in conjunction with PRS is uncertain, but has been reported to range from 36.6% to 53.6%22,23. According to Tollefson and Witman22, 15 cases (53.6%) among 28 PRS patients were associated with en coup de sabre. This relatively common coexistence lead them to believe that both disease may share a similar pathogenesis. In addition to these previous studies, the patients described herein displayed both diseases; therefore, we agree with that opinion.
However, even though several cases of PRS accompanied by en coup de sabre have been reported, en coup de sabre with bilateral involvement as in the second case described herein is very rare. In a study conducted Tollefson and Witman22, among 54 patients diagnosed with PRS or en coup de sabre, only one patient had en coup de sabre on one side and PRS on the other. Among the cases of PRS available in the Korean medical literature, only four cases were accompanied by en coup de sabre, and no case showed bilateral involvement24-27.
In conclusion, the clinicopathological similarity of PRS and en coup de sabre and the frequent coexistence of these two diseases in the same patients support our assertion that both diseases are on the same spectrum as the variants of localized scleroderma.



 XML Download
XML Download