

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dermatofibroma (DF) is perhaps the most common mesenchymal growth of the skin. It has a predilection for the lower legs of women in their early 20s. This tumor most frequently occurs in the dermis with or without extending into the subcutaneous tissue1. The benign DF is usually confined to the dermis, whereas the occurrence of this lesion purely in the subcutaneous tissue has uncommonly been reported2-5. According to the WHO, a deep location is found for less than 1% of all benign fibrous histiocytomas5. Herein, we report an uncommon case of a purely subcutaneous DF.
CASE REPORT
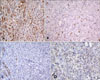
A 41-year-old male presented to our dermatology outpatient clinic, with an apparently asymptomatic palpable subcutaneous skin lesion on the left thigh, appearing 3 months prior to his visit to our clinic. There was no previous history of medication use or trauma and no family history of skin disease. The lesion was a hard, solitary, discrete, subcutaneous papule. The lesion had not been increasing in size over the last 3 months. The hard subcutaneous papule popped out when an incision for biopsy was made into the skin above the lesion. Histologic findings showed a well-circumscribed, subcutaneous papule composed of fibrohistiocytic proliferation (Fig. 1A). Storiform arrangement of spindle cells, trapping normal collagen bundles at the periphery of the lesion were consistent with subcutaneous DF (Fig. 1B). There was no nuclear pleomorphism or hyperchromasia (Fig. 1C). Immunohistochemical staining demonstrated positivity for factor XIIIa (polyclonal, dilution 1:200, Biogenex, Fremont, CA, USA) (Fig. 2A), and negativity for CD34 (monoclonal, clone QBEND 10 dilution 1:50, Dako, Carpinteria, CA, USA) (Fig. 2B), desmin (monoclonal, Clone D33 dilution 1:20, Dako) (Fig. 2C). CD68 (monoclonal, clonePG-M1 dilution 1:50, Dako) staining showed negative reactions in the spindle cells (Fig. 2D). Microscopic and immunohistochemical examinations confirmed the diagnosis of subcutaneous DF. The patient is asymptomatic with no evidence of recurrent disease at the 3-year follow-up.
DISCUSSION
Our case showed strong immunohistochemical positivity for factor XIIIa (polyclonal, dilution 1:200, Biogenex) and negativity for CD34 (monoclonal, clone QBEND 10 dilution 1:50, Dako), desmin (monoclonal, Clone D33 dilution 1:20, Dako) and CD68 (monoclonal, clonePG-M1 dilution 1:50, Dako) staining showed negative reactions in the spindle cells.
It is important to recognize the pure subcutaneous variant of DF because it may be confused with a variety of benign and malignant subcutaneous tumors6. Among the benign subcutaneous tumors, deep penetrating dermatofibroma (DPDF) or dermatofibroma extending into the subcutaneous tissue was described as a variant of dermatofibroma by Kamino and Jacobson7 in 1990. Kamino and Jacobson7 published the histologic criteria to distinguish DPDF from dermatofibrosarcoma protuberans (DFSP). Scanning magnification is the most helpful tool in distinguishing a regular, smooth, nodular or scalloped pattern of demarcation in DPDF from the irregular, lacelike/honeycomb or multilayered pattern of DFSP8. In previous reports, most cases of DPDF were positive for factor XIIIa and negative for CD34 and vice versa in cases of DFSP.
Malignant fibrohistiocytic neoplasms are composed of malignant pleomorphic sarcomatous cells, bizarre giant cells, and frequent mitotic figures. Histological features, unfortunately, play a minor role in predicting the biologic behavior of these neoplasms9. The presence of certain atypical histological features, including necrosis, marked cellular and mitotic activity, does not correlate well with clinical recurrence.
As with benign fibrohistiocytic neoplasms, the diagnosis of malignant fibrohistiocytic neoplasms frequently relies upon electron microscopy and immunohistochemistry to differentiate it from other lesions. Like DF, DFSP occurs in the dermis and subcutis, but is more apt to show extensive subcutaneous involvement than benign DF. It is also characterized by a more uniform cellular population and lacks giant cells, inflammatory cells, and xanthomatous elements. Its fascicles, composed of slender attenuated cells, are longer and arranged in a distinct storiform pattern, unlike the short curlicue fascicles of DF. Its margins are infiltrative in contrast to the well-defined margins of DF10,11. However, DFSP may be difficult to differentiate from DF. Immunostaining can help to reveal the distinct differences in the cellular composition of these tumors. DF contains a significant population of factor XIIIa-positive cells, although it has been debated whether these cells represent a population of neoplastic cells or a peculiar infiltrate that accompanies the tumor. In contrast, DFSP contains only scattered factor XIIIa-positive cells, but, in striking contrast to DF, it expresses CD34 in a significant portion of neoplastic cells12,13. The combination of these two stains has proved to be highly reliable in distinguishing these two lesions, which often cause diagnostic problems, particularly when only a superficial biopsy specimen is available for assessment.
Usually, DF does not require treatment unless it is symptomatic. As per the literature, most subcutaneous DF's were treated by local excision without sacrificing structures that would cause major functional or cosmetic morbidity. Our patient had not symptom but the lesion was removed when an incision for biopsy was made into the skin above the lesion.
DF almost pursues a benign course, with a recurrence rate of less than 2%, although a higher rate of recurrence has been reported for some variants, including the cellular, aneurysmal, and atypical (pseudosarcomatous) forms14. A higher rate of recurrence has been noted in the subcutaneous and deep types and in lesions located on the face, in which a recurrence rate of 15% has been reported6,15. Also, a local recurrence rate of 19% (four of 21 cases) has been reported in 21 cases from the previous subcutaneous DF series2. Accordingly, if the lesion has been proved to be subcutaneous DF with or without symptoms, it would seem reasonable to recommend that the lesion should be completely removed by local excision. In this paper, we have reported an uncommon case of subcutaneous DF.

 XML Download
XML Download