

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Melanocytic nevi appear in a wide morphological variety. Several clinical types including flat lesions, slightly elevated lesions often with a raised center and a flat periphery, papillomatous lesions, dome-shaped lesions, and pedunculated lesions have been previously reported1. Melanocytic nevi are subject to change with age in both clinical and histopathologic findings2.
CASE REPORT
Case 1
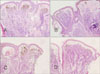
A 31-year-old female patient presented with a tumor on her back. She was born with the skin lesion which had slowly been protruding from the skin surface. The lesion was a 3.0×2.5 cm sized brown to black tumor that contained a slight hair growth (Fig. 1A). A punch biopsy specimen revealed an intradermal nevus with aggregated nests of nevus cells in the dermis. In some areas, the nevus cells were replaced by fat cells that were irregularly distributed throughout the dermis (Fig. 2A). Fibrotic collagen changes and neuroid degeneration were also shown.
Case 2
A 29-year-old female patient had a congenital skin lesion on her abdomen. Physical examination showed a 1.2×0.7 cm sized dark brown tumor with a few satellite lesions (Fig. 1B). A punch biopsy revealed the histologic pattern of intradermal nevus with slight neurotization and fibrosis. There was sparse fatty degeneration. Its rete ridges were fused to form an isolated space filled with nevus cells (Fig. 2B).
Case 3
A 29-year-old female patient visited our clinic with a congenital skin lesion on her chest. Physical examination revealed a 2.0×1.6 cm sized lobulated raspberry-shaped tumor that was dark brown color (Fig. 1C). The tumor had been enlarging slowly. A punch biopsy was done and histologic findings revealed the architecture of an intradermal nevus with isolated space filled with nevus cells (Fig. 2C).
Case 4
A 21-year-old female patient presented with a slowly growing tumor on the posterior aspect of the scalp. The lesion was a 1.5×1.5 cm brown to black colored raspberry-shaped tumor that contained a slight hair growth (Fig. 1D). A punch biopsy specimen revealed an intradermal nevus with aggregated nests of nevus cells in the dermis. Fibrotic changes were apparent in some area. There was sparse fatty degeneration (Fig. 2D).
DISCUSSION
In 1991, Cho et al.3 reported three cases of intradermal nevi with an unusual growth pattern and appearance, and which differed from previously described clinical types. The lesions clinically showed lobulation and histologically exhibited findings in common; that is, scattered fat cell infiltration within nests of nevus cells, neuroid differentiation of nevus cells, and dermal fibrosis. Although they looked similar to previous disease entities, including nevus lipomatous superficialis and cerebriform nevus, they could be distinguished based upon histopathological findings. Nevus lipomatous superficialis demonstrates groups or strands of fat cells instead of scattered ones8, and cerebriform nevus dose not reveal fatty degeneration or fibrosis9. Therefore they named the lesions "lobulated intradermal nevus" and suggested their cases represented an unusual form of regressing melanocytic nevus.
Reviewing all the cases reported in the context of lobulated intradermal nevus, their manifestation is slightly heterogeneous (Table 1). Our first case was composed of irregularly sized lobules and it looked like those of Cho et al.3, Lee et al.6 and Löffler and Effendy7. Löffler and Effendy7 reported this grape-like clinical variant under the name of corymbiform nevus. Though Lee et al.6 reported the case as lobulated intradermal nevus, we think it differed a little from other cases of lobulated intradermal nevus because there is no fat cell infiltration. Our other cases were raspberry-shaped tumors, which generally are protruding tumors with raspberry-like surface made up of multiple small papules; there has been one more case like this in previous literature3. Most previously reported cases were lobulated intradermal nevi of verrucose plaque type, showing a generally flat plaque with verrucose surface3-5. So we suggest that lobulated intradermal nevus has at least 3 different clinical types, including corymbiform, verrucose plaque and raspberry-like type.
In this case series, we reported four lobulated intradermal nevi which developed in female patients. Interestingly, all the previous seven cases were also reported in women3-7. The sexual predominance implies that lobulating changes might be associated with factors such as female hormones, however, further studies are required to clarify the association.
The patients who had lobulated intradermal nevus were in their twenties or early thirties, and the duration of nevi ranged from approximately 20 to 30 years. Similarly, previous cases had existed for 20 to 40 years when found3-7. Therefore, we believe that these changes require a long time to develop.
In 2007, Yus et al.10 introduced a classification of acquired intradermal nevus: Unna's nevus and Miescher's nevus. Clinically, Unna's nevus is an exophytic soft nevus, predominately located on the neck, trunk, and limbs, and Miescher's nevus is a dome-shaped nevus, predominately located on the face. In the context of this classification, all reported cases of lobular intradermal nevus may look like Unna's nevus. But there is a limitation for the application of this classification to lobulated intradermal nevus. The classification of Yus et al.10 is confined to an acquired type. However, most of the reported cases of lobulated intradermal nevus are congenital types. Although one of the cases of Cho et al.3 is reported to be an acquired type, there is a possibility of unrecognized congenital nevus because of long duration of disease (30 years).
Histopathologic changes associated with aging of melanocytic nevi, such as, fatty degeneration, fibrosis, and neural changes, are found in lobulated intradermal nevus11. Cho et al.3 hypothesized that these histopathologic changes resulted in continuous enlargement and lobulating appearance of melanocytic nevi. Our cases also showed all these changes in a variable degree. In conclusion, we agree to the former opinion and suggest that lobulation is a rare clinical manifestation which is associated with common histopathologic findings of aging melanocytic nevi. And we also think that lobulated intradermal nevi are both clinically and histopathologically heterogenous entities. Their clinical and histopathologic changes are variable in degree but on a collinear spectrum.
Herein we report a case series of lobulated intradermal nevus, another clinical variant which is rare and interesting.


 XML Download
XML Download