

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Syringoma is a relatively common appendageal tumor that shows eccrine acrosyringeal differentiation. Eccrine ducts are widely distributed in the skin. However, syringomas are usually found in the head and neck region, and most often on the eyelids1. Less commonly, they can be seen on the scalp, forehead, cheeks, abdomen, extremities, genitalia and buttocks2. Limited distributed syringoma around the axilla is a very rare phenomenon. We report here on a rare and interesting case of axillar syringoma.
CASE REPORT
A 24-year-old woman presented with a 2-year history of asymptomatic papules on both her axillae. She was otherwise healthy, and there was no family history of skin lesions. On the physical examination, there were multiple 1 to 3 mm light-brown papules on both axillae (Fig. 1). They were not associated with the roots of hairs. There were no papules on her eyelids.
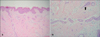
We performed a 4-mm punch biopsy. The histopathologic findings of the papule biopsy showed multiple ductal and small cystic structures embedded in a fibrous connective tissue stroma in the dermis. The ducts were lined by 1 or 2 rows of epithelial cells (Fig. 2). These histopathologic findings were consistent with syringoma. The patient has been treated with topical tretinoin, but the lesions have not responded.
DISCUSSION
Syringomas are benign sweat gland tumors that originate from the straight portion of the intradermal eccrine sweat duct. Eccrine sweat ducts are distributed widely in the skin. However, these tumors are usually found in the head and neck region, and most often on the eyelids1. Less commonly they can be seen on the scalp, forehead, cheeks, abdomen, extremities, genitalia and buttocks2. They clinically present as small, firm, skin-colored, yellow or brown papules3. Syringomas are encountered more frequently in women with a female to male ratio of approximately 2:1 according to most studies, although some quote a ratio as high as 6.6:14,5. They most often occur during puberty or during the third and fourth decades of life2. There is a more rare eruptive form in which the lesions present in large numbers and in successive crops on the anterior chest, neck, upper abdomen, axillae and periumbilical region2,4.
There is some debate over the eccrine origin of syringomas as most of them are located in apocrine rich areas such as the lower eyelid, axillae and abdomen, and they rarely occur in eccrine only areas like the palms and soles6. However, immunohistochemical studies have shown the presence of several enzymes, including succinic dehydrogenase, aminophosphorylase, periodic acid-Schiff-positive material and leucine aminopeptidase, and all of which are more highly concentrated within the eccrine ducts as compared to apocrine glands7. Current evidence supports the theory that syringomas may be under hormonal control; several immunohistochemical studies have detected progesterone and estrogen receptors within these tumors. The presence of these hormone receptors may explain why syringomas are more common in females and they have a peak incidence during puberty8. Furthermore, there are reports that have shown an increase in tumor size during pregnancy and menstruation3. Yet a recent study on 63 patients with syringoma described only one patient who experienced an exacerbation of her symptoms during menstruation5. Our patient also showed no change in tumor size during menstruation.
Making the clinical diagnosis is not difficult for the cases with a typical location of syringoma. Yet the diagnosis is likely to depend on the histologic findings in those cases without typical facial involvement. Axillary syringoma should be differentiated from other diseases that present with brown popular lesions in the axillae such as Darier disease, Fox-Fordyce disease, Hailey-Hailey disease, flat wart and keratosis pilaris9. Darier disease affects several areas simultaneously such as the axillae, upper chest area, back, ears, nasolabial folds, forehead, scalp and groin. The lesions of Darier disease can be greasy, scaly, crusted, and keratotic. Patients with Darier disease also show characteristic nail changes9. Hailey-Hailey disease has a varied morphology, but in general it is a blistering disease that can present with episodic macerations and erosions in the intertriginous areas. The lesions of Fox-Fordyce disease are small infundibulocentric papules that may have a central keratotic plug and yellow color10.
The clinical appearance of our patient was quite unusual as the cutaneous manifestation presented as light-brown papules limited to the axillae. We could find no similar case of syringoma in the medical literature. So, physicians should recognize the various clinical presentations of syringoma, and syringoma should be considered when making the differential diagnosis of popular lesions on the axillae.

 XML Download
XML Download