

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Robinson1 was the first to describe eccrine hidrocystoma (EH) in 1893. EHs characteristically appear as skin-colored to bluish vesiculopapular lesions, and most commonly on the periorbital area, and these lesions predominantly occur in middle-aged and elderly women2,3. EH is a benign small cystic lesion that usually enlarges during the summer and may disappear spontaneously in cooler weather2. To the best of our knowledge, EH in children has not previously been described in the medical literature and grouped EHs localized on the tip of the nose is a very rare and atypical presentation.
CASE REPORT
An 8-year-old boy presented with a 3-year history of multiple flesh-colored to bluish domed papules on the tip of the nose (Fig. 1). CO2 laser treatment had been performed at a local clinic during the prior year, but the lesions had not completely resolved. Both his past medical and family histories were not remarkable. The papules became more prominent in hot environments.
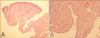
The histopathology showed a dilated, partially cystic structure in the middermis (Fig. 2A). The cystic cavity was lined by one or two layers of cuboidal or flattened epithelial cells (Fig. 2B). No decapitation secretion was visualized. The immunohistochemical studies showed positivity for CEA, but negativity for S-100 and PAS (Fig. 3). The diagnosis of EH was established based on these findings.
Therapy with topical 1% atropine sulfate two times daily was instituted. The skin lesions showed great improvement after a month of treatment. No recurrence has been noted during the 1 year follow-up period.
DISCUSSION
EH usually presents as a small, translucent, cystic nodule that is 1 to 3 mm in diameter and the nodule often has a bluish hue3. They are predominantly found on adult females, they occur as single or multiple lesions and they are mostly located on the periorbital and malar regions2. EH is prevalent in adults between the ages of 20 and 70 years2,4. There have been no reported cases of EH in childhood in the medical literature.
EH is currently classified into two types according to the number of lesions. The first type was described by Robinson1 and this is known as the Robinson type. Most of his patients were women who worked in hot and humid environments. Their lesions were characterized as having multiple small papules1. Smith and Chernosky5 subsequently described a group of patients whose lesions were primarily solitary. The individual lesions of the multiple type are similar to the solitary lesions of the Smith type, except they are smaller6. Tokura et al.7 suggested solitary EH is derived from the secretory coil, and the multiple ones are derived from the duct. The Robinson-type multiple EHs are much more common in Korea and the Smith-type solitary EHs are relatively rare4.
The etiology of multiple EH remains unknown. A suggested cause for EH involves occlusion of the intradermal portion of the eccrine duct8. However, Murayama et al.9 suggest that EH is a hamartoma-like disorder that becomes more pronounced as a result of retaining sweat. We thought that the latter hypothesis might explain the atypical, early presentation of our case.
EH must be differentiated from apocrine hidrocystomas. Apocrine hidrocystoma is usually larger and it does not become more prominent in hot environments or after exercise10. Apocrine hidrocystomas affect the same age groups as do EHs, and they rarely occur during childhood or adolescence2. Histopathologically, eccrine hidrocystoma, which is lined by ductal cells, differs from apocrine hidrocystoma by the absence of decapitation secretions, papillary projection into the lumen, PAS-positive granules and myoepithelial cells. EH is usually unilocular, whereas apocrine hidrocystomas are multilocular2. Histochemically, solitary EH stains positive for S-100 protein, whereas the Robinson type EH and apocrine hidrocystomas do not2. However, it may be difficult to differentiate EH from apocrine hidrocystomas even with conducting immunohistochemical study2,11.
There is an interesting previously reported case of steatocystoma multiplex localized on the nose of a child12. But the differentiation with EH was not difficult because steatocystoma usually has a yellowish color and it is histopathologically characterized by a folded cyst wall that consists of squamous epithelium, flattened sebaceous lobules within or close to the wall and a positive reaction of the lining cells for PAS. Clinically, other cystic lesions such as epidermal inclusion cyst, comedone and mucous cyst could be considered in the differential diagnosis, but all these lesions differ from EH histopathologically13-15.
Although a solitary EH can be easily treated with surgical excision, eliminating multiple hidrocystomas is difficult because of their number and cosmetic location. The therapeutic options can be divided into medical and surgical modalities. Multiple lesions have been treated with topical scopolamine, topical atropine and botulinum toxin type A16,17. Simple needle puncture has not been shown to produce lasting effects18. Using a 585-nm pulsed dye laser has resulted in good outcomes when treating multiple EHs19. Most importantly, avoiding hot temperatures or humid conditions will help prevent worsening of symptoms in patients. We chose topical atropine as a treatment method because of the patient's young age, and the number of skin lesions, and the site of presentation was cosmetically and functionally important.
The age at presentation and the clinical features of our case do not mimic the classic presentation of EH, be it the Robinson-type or the Smith-type. Due to the histologic findings, the lesion's aggravation during hot weather and the good response to atropine sulfate, we were able to make the diagnosis of EHs with an atypical presentation.


 XML Download
XML Download