

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tumors with hair follicular differentiation are difficult to differentiate due to the variety and similarity of the
lesions. Trichogerminoma is an uncommon tumor that originates from hair germ cells and it was first reported on
by Sau et al.1 in 1992. Kazakov et al.2 showed the immunohistochemical uniqueness of trichogerminoma and the tumor was confirmed as being a unique entity, yet there is still controversy about this. Therefore, additional observation and research are needed to clarify its features. We report here on a case of trichogerminoma that developed on the nape of the neck of an elderly woman. We believe this is the first reported case of trichogerminoma in the Korean dermatological literature.
CASE REPORT
A 79-year-old woman presented with a 5-year history of an asymptomatic solitary nodule on the left posterior neck. It was a non-ulcerated, hemispheric, well-demarcated, movable nodule with no subjective symptoms (Fig. 1). The clinical diagnosis was epidermal cyst.
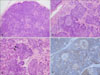
Excisional biopsy was performed and the lesion was totally removed. The gross examination of the surgical specimen demonstrated the mass to be 10×10 mm in size with a maximum depth of 8 mm. There was no internal necrosis or hemorrhage. Histological examination revealed a sharply demarcated, deep dermal and subcutaneous tumor surrounded by a pseudocapsule (Fig. 2A). The tumor had no connection to the overlying epidermis and the tumor consisted of variously sized nodules separated by a fibrocytic stroma. There was no cleft between the tumor nodules and stroma. The nodules were composed of smaller lobules that were made up of basophilic cells. Characteristically, within most of lobules, round nests or cell balls formed by dense, concentrically arranged basaloid cells were seen. Pale cells with prominent large nuclei and dispersed chromatin occupied the central area of the nests (Fig. 2B). Typical mitoses were frequently present in these areas. The outer layer of the lobules was composed of undifferentiated columnar basophilic cells that displayed peripheral palisading.
In some areas, cords of germ cells extended from the periphery of the lobules and formed buds into the stroma. In other areas, the basaloid cells showed keratinization with pyknotic nuclei and nuclear debris near the center of the lobule that resembled infundibular epithelium and these cells had developed keratinous microcysts (Fig. 2C).
On the immunohistochemical examination, the tumor cells showed CK5/6 and p63 immunoreactivity, and they stained negatively for carcinoembryonic antigen (CEA). The peripheral rims of the cell balls were prominently stained with anti-CK5/6, whereas the center of the cell balls showed weaker staining with anti-CK5/6 (Fig. 2D). Most of the tumor cells were strongly stained with anti-p63 (data not shown). The dendritic cells scattered within the lobules and the stroma showed reactivity for S-100. The peripheral tumor cells and the hyaline-like thin membrane around some lobules were positive on periodic acid-Schiff staining.
There was no recurrence of tumor during 6-months follow up after complete excision.
DISCUSSION
Trichogerminoma is a rare tumor of hair germ epithelium, and it was first described by Sau et al.1 in 1992. Most cases manifest as an asymptomatic solitary, slowly growing, deep-seated nodule, and the sizes vary from 7 to 40 mm. It shows a male predominance and it generally occurs in middle-aged individuals. The involved sites are mostly on the face and less frequently on the scalp, trunk and extremities.
Histological examination reveals a well-demarcated dermal-subcutaneous nodule composed of smaller lobules with basaloid cells. The tumor cells are uniformly basophilic cells with round nuclei, dispersed chromatin and a tendency to show peripheral palisading. The distinctive feature of this tumor is "cell balls" that resemble hair bulbs, and these are concentrically arranged clear cells and peripheral condensation with little or no intervening stroma in some lobules. In the eccentric areas of the cell balls, the basaloid cells may present keratinization and they develop keratin microcysts that resemble abortive hair bulbs. In some areas, the tumor cells extending from lobules make anastomosing strands or buds. The various other histological features of this tumor include clear cell change that is suggestive of differentiation towards the outer root sheath of hair follicles and divergent sebaceous differentiation. The stroma is fibrocytic, and there is no retraction cleft between the lobules and stroma. Our case displayed several features of hair follicular differentiation, including the characteristic 'cell balls', cords of basaloid cells and keratin microcyst formation1-4.
Immunohistochemically, the tumor cells express a ring-like staining pattern of cytokeratin markers such as AE1/AE3, CK5/8 and CK5/6 with prominent immunoreactivity in the peripheral rims of the lobules2,3. These results may reflect outer root sheath differentiation5. As in other hair germ neoplasms, dendritic S-100 protein positive cells are scattered within the tumor. Sebaceous glandular differentiation can be defined by the epithelial membrane antigen and CEA staining3. CK20-positive Merkel cells are not found in the epidermis overlying the tumor. Periodic acid-Schiff stain reveals vitreous layer-like eosinophilic membranes surrounding many cell groups. Our case demonstrated the distinctive ring-like pattern of cytokeratin staining, which helped make the diagnosis of trichogerminoma. We studied the p63 immunoreactivity to clarify the differentiation potential of the tumor cells. However, there was no regional difference in the staining pattern between the two types of tumor cells, and p63 showed strong immunoreactivity in all tumor cells, the same as in other pilar tumors. In the hair follicle-derived tumors, the cell components originating from the outer root sheath cells or matrix cells expressed p636.
There is still debate among dermatopathologists about trichogerminoma, and some consider it to be part of the spectrum of trichoblastoma. However, trichogerminoma differs from trichoblastoma in that it differentiates toward various pilosebaceous structures. In addition, trichoblastoma shows a different immunohistochemical pattern such as CK20-positive Merkel cells in the tumor and the overlying epidermis7, a half-moon pattern of calretinin-positive tumor cells in almost every epithelial aggregation and the lack of zonal CK5/6 immunostaning8,9. Tumors of basaloid cells or hair follicular differentiation need to be differentiated from trichogerminoma. Trichoblastoma is made up of basaloid cells, but they display less advanced hair differentiation than trichogerminoma. The centrolobular areas of clear cells have been observed in trichoblastoma8, but this pattern is not a dominant microscopic feature. Trichoepithelioma is a tumor that is made up of islands of basaloid cells with peripheral palisading and it has characteristic keratin cysts. Unlike trichogerminoma, it shows no nests of concentric pale cells. Trichilemmoma is characterized by periodic acid-Schiff positive glycogen rich clear cells and palisaded columnar cells at the periphery that rest upon a thickened basement membrane. Basal cell carcinoma with follicular differentiation is a tumor with basaloid cells budding from the epidermis or follicles with a horn cyst resembling a follicular structure. However, it shows a lack of papillar formation and there are no centrolobular balls of concentric pale cells. The different characteristics of each tumor from trichogerminoma are summarized in Table 17,10.
Trichogerminoma has a benign course. All the cases, except for one case of undifferentiated carcinoma that developed from trichogerminoma and that ended in death due to metastasis and progression of the disease, have shown no recurrence after surgical removal1-4. Because of the potential of malignancy, complete excision of the tumor should be the treatment of choice.


 XML Download
XML Download