

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Desmoid tumors are benign tumors exhibiting fibroblastic proliferation that arise from fascial or musculoaponeurotic structures. They are rare in the general population, accounting for 0.03% of all neoplasm, although they occur more commonly in familial adenomatous polyposis (FAP)patients, exhibiting an incidence of 3.5~32%, and the incidence is 29% in the original Gardner kindred1
,2.
Gardner's syndrome is an autosomal dominant inherited condition, characterized by polyposis coli, osteoma and various soft tissue tumors, including desmoid tumors. We herein report a woman with Gardner's syndrome associated with desmoids tumor.
CASE REPORT
In January 2008, a 16-year-old girl visited our clinic complaining of a palpable mass on right subscapular area developed since birth. She was under evaluation with incomplete development of teeth at the oral surgery department, and was referred to our department to evaluate the skin tumor. The patient had been in her usual state of health, and had no remarkable past medical history. None of her family members had known health problems or any hereditary diseases.
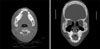
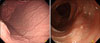
Skin examination revealed a non-tender, hard, skin colored, elevated and well-confined mass on the right subscapular area, measuring 7×4 cm (Fig. 1). All laboratory examinations on blood and urine were within the normal limits. Computer tomography of the oropharynx showed polyostotic fibrous dysplasia involving facial, skull base and cranial bones (Fig. 2). Gastrofibroscopy and colonoscopy revealed numerous small polyps in the stomach and colon (Fig. 3). Polyps in colon were tubular adenomas histopathologically.
Skin biopsy was performed in the middle of the subscapular mass, which showed dense collagen bundles in dermis, and among thickened collagen bundles were ongoing fibroblasts normal differentiation (Fig. 4). Cytogenetic studies showed nonsense mutation of the APC gene on the 4,585th base sequence of exon 15. Studies on her family members were not performed.
Finally, she was diagnosed with the Gardner's syndrome according to fibrous dysplasia of facial bone, polyposis of stomach and colon, subscapular desmoid tumor and mutation of APC gene. She is now under observation with periodic colonoscopy, without any progression of disease so far.
DISCUSSION
Gardner's syndrome was first reported by Gardner and Smith in 1958. It is an autosomal dominant, non-sex linked, complex condition involving soft-tissue masses, bony tumors, and polyposis coli1,3. It is considered to be a variant of FAP, as both entities are caused by mutations in the APC gene located at band q21 on chromosome 5, of which 20% are de novo in nature4.
Extracolonic manifestations include osteomas involving the maxilla, the mandible, long bones, cranial bones and the sinuses, epidermoid cysts, lipomas, dental anomalies such as impacted and supernumerary teeth. There are also central nerve system tumors, thyroid gland adenomas and carcinomas, adrenal gland adenomas and carcinomas, upper gastrointestinal polyps, duodenal, pancreatic, liver and biliary neoplasm, carcinoid of the small bowel, lymphoid hyperplasia of the terminal ileum and congenital hypertrophy of the retinal pigment epithelium5, and desmoids tumors.
About 2% of desmoid tumors are FAP-associated, and patients with FAP are at 852 times the risk of developing desmoids tumors in the general population2. Although etiological factors in desmoids tumors are unclear, three factors including, initiation of trauma, influence of sex steroids and an underlying genetic defect, have been implicated in the etiology of desmoids tumors2.
Based on their location, desmoids tumors can be divided into three types, intra-abdominal, abdominal wall and extra-abdominal, in order of frequency. Symptoms depend on the location of the tumor. Many studies have shown that between 37% and 50% of desmoids arise in the abdominal region6. Intra-abdominal desmoids can remain asymptomatic for a considerable period, while relentlessly enlarging and infiltrating adjacent structures causing intestinal, vascular and urinary obstruction or neural involvement7. The most common extra-abdominal sites include the shoulder girdle, chest wall and inguinal regions. Pathologically, desmoids tumors are similar to other fibromatoses, including scar hypertrophy, mesenteric fibromatosis, Dupuytren's contracture, and low grade sarcoma. They are arising from the musculoaponeurotic soft tissues, and composed of well-differentiated and uniform collagenous fibroblasts and fibrocytes. They are locally invasive but do not metastasize2,6-8.
Because Gardner's syndrome is characterized by colorectal cancer in early adult life secondary to extensive adenomatous polyps of the colon, patients need to undergo surgery. Total proctocolectomy with ileostomy or colectomy with ileorectal anastomosis is recommended5,9. Treatment of desmoids tumor is controversial. Although surgery is widely accepted as the first line treatment, the high recurrence rate has led some authors to suggest that surgery should be avoided, except for bypass of bowel obstructions or relief of ureteric obstructions caused by intraabdominal desmoids tumors. Pharmacological pain control with non-steroid anti-inflammatory drugs and anti-estrogen agent is the most widely documented management. Chemotherapy and radiotherapy are also alternatives considered in symptomatic patients who do not response to conventional medical therapy2,10.
As far as we know, a 55-year-old woman has been reported as Gardner syndrome associated with desmoids tumor so far who experienced FAP, osteomatous jaw and ocular lesion, numerous dental abnormalities and abdominal tumor11. Our patient had fibrous dysplasia of the facial bone, polyposis of stomach and colon, and subscapular desmoid tumor revealing mutation of APC gene. We report this 16-year-old woman with Gardner's syndrome complicated by desmoid tumors on the right subscapular area, a rare case in Korea.


 XML Download
XML Download