

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Psoriasis is a chronic immune-mediated inflammatory disorder that affects nearly 1.5~3% of the world's population. Psoriasis manifests as skin lesions with typical silvery scales and, potentially, by arthritis1-3. Recent studies have demonstrated an association between systemic inflammatory diseases such as psoriasis, systemic lupus erythematosus or rheumatic arthritis and the cardiovascular risk factors, including metabolic syndrome4. Inflammatory cytokines such as tumor necrosis factor (TNF) play an important role in the pathogenesis of both psoriasis and metabolic syndrome. Previous reports have shown an association between psoriasis and diabetes, hypertension, obesity, myocardial infarction and heart failure3,5-7. Systemic medications such as acitretin, cyclosporine and methotrexate, which are used to treat psoriasis, can increase the risk of cardiovascular diseases by inducing hypertension, hyperlipidemia and so on8-10. However, there is no published study that has focused on the association between psoriasis and cardiovascular diseases and their risk factors in Koreans. To demonstrate the relationship of psoriasis with the cardiovascular risk factors, we assessed the presence of cardiovascular risk factors, metabolic syndrome and cardiovascular diseases in patients with psoriasis and in control subjects.
MATERIALS AND METHODS
Patients and controls
We performed a case-control study with the data collected from Hallym Sacred Heart Hospital between 2007 and 2009. The patients with psoriasis were defined as having been diagnosed by histopathological examination, they had to be 15 years of age or older and they visited the Department of Dermatology, Hallym Sacred Heart Hospital. The control group consisted of randomly selected subjects who had visited the hospital's Health Promotion Center with neither a history of a diagnosis with psoriasis nor a coded ICD-10-CM diagnosis of psoriasis.
Methods
The smoking status and medical problems, including cardiovascular diseases, hypertension, diabetes and hyperlipidemia, were surveyed. The height, body weight, waist circumference, blood pressure, fasting plasma glucose and the serum lipid profiles were measured in both the patients with psoriasis and the controls. We also investigated the duration, family history and type of psoriasis for the patients with psoriasis. We defined the patients as having moderate to severe psoriasis if they had a history of systemic treatments consistent with a moderate to severe state of disease, such as acitretin, etretinate, cyclosporine, methotrexate, mycophenolate, biologics or phototherapy. We defined the patients who had received only topicals such as steroids or vitamin D derivatives as having mild psoriasis. We excluded the patients with mild psoriasis and who had been unable to receive systemic treatment because of their old age, a general poor condition or infection.
Diagnostic criteria of metabolic syndrome
According to the diagnostic criteria revised by the International Diabetes Federation (IDF) in 200411, metabolic syndrome was defined as central obesity (according to the ethnicity-specific waist circumferences) plus any 2 of the following criteria. (1) increased triglycerides (TG): ≥150 mg/dl (1.7 mmol/L) or specific treatment for this lipid abnormality. (2) Reduced high-density lipoprotein (HDL) - cholesterol: <40 mg/dl (1.03 mmol/L) in men and <50 mg/dl (1.29 mmol/L) in women or specific treatment for this lipid abnormality. (3) Increased blood pressure: systolic >130 mmHg or diastolic >85 mmHg or treatment for previously diagnosed hypertension. (4) Increased fasting plasma glucose: fasting plasma glucose >100 mg/dl (5.6 mmol/L) or previously diagnosed type 2 diabetes. In this study, we defined central obesity as a waist circumference >90 cm in men and >85 cm in women according to the diagnostic criteria of metabolic syndrome in Koreans12.
Evaluation of the cardiovascular risk
Cardiovascular diseases, metabolic syndrome and cardiovascular risk factors such as smoking, obesity (body mass index [BMI] >25), hypertension, diabetes and hyperlipidemia were compared between the patients with psoriasis and the controls. The Framingham 10-year risk score13, which was designed to estimate the 10-year risk for major coronary events in adults aged 20 and older and who do not have heart disease or diabetes, was calculated for the patients with psoriasis. By applying the National Cholesterol Education Program's (NCEP) adult treatment panel III (ATP III) guideline14 on the basis of the Framingham 10-year risk score and the cardiovascular risk factors, we determined if the patients with psoriasis needed lifestyle changes and/or drug therapy to maintain proper LDL levels.
Statistical analysis
Chi-square tests and student's t-tests were used to determine the statistical significance of the differences of age, gender, smoking, obesity, cardiovascular diseases, hypertension, diabetes, hyperlipidemia and metabolic syndrome between the patients with psoriasis and the controls. Chi-square tests and logistic regression analysis were used to determine the risk factors for metabolic syndrome in the patients with psoriasis. All the statistical analyses were performed using SPSS (Windows version 13.00; SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
RESULTS
Demographic data of the subjects
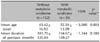
A total of 197 patients with psoriasis and 401 controls were included in this study. In the patient group, there were 114 men (57.9%) and 83 women (42.1%). In the control group, there were 243 men (60.6%) and 158 women (39.4%). There were no significant differences in gender between the groups (p=0.522). The mean age of the patient group was 45.04±16.64 years (mean±SD) and that of the control group was 46.89±14.62 years (mean±SD). There were no significant differences in the mean age (p=0.186) and the distribution of age (p=0.125) (Table 1).
Metabolic syndrome, cardiovascular diseases and the risk factors
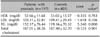
The prevalence of metabolic syndrome was 17.8% (n=35) among the patients with psoriasis and 11.0% (n=44) among the controls (p=0.021). The prevalence of cardiovascular diseases was 4.6% (n=9) among the patients with psoriasis and 1.7% (n=7) among the controls (p=0.044). The cardiovascular diseases in the patients with psoriasis were myocardial infarction (n=1), unstable angina (n=2), stable angina (n=2), heart failure (n=3) and arrhythmia (n=1). We observed a higher prevalence of smoking, obesity, hypertension, diabetes and hyperlipidemia in the patients with psoriasis, as compared with that of the controls. However, significant differences were only observed for hypertension (32.5% of the patients, 13.7% of the controls, p=0.000) and hyperlipidemia (22.3% of the patients, 15.0% of the controls, p=0.025) (Table 2).
Serum lipid profiles
TG was significantly increased in the patients with psoriasis (152.17±76.44 mg/dl) as compared to that of the controls (119.16±70.32 mg/dl) (p<0.001). There were no statistically significant differences in total cholesterol, HDL and LDL cholesterol (Table 3).
Risk factors for metabolic syndrome in the patients with psoriasis
We found that the significant risk factors for metabolic syndrome in the patients with psoriasis were age (p<0.05), a family history of psoriasis (p<0.05) and the severity of psoriasis (p<0.01) (Table 4). There was no gender-related predominance of metabolic syndrome in the patients with psoriasis. Metabolic syndrome was not found in the psoriasis patients who were 11~29 years old. The highest prevalence of metabolic syndrome was observed in the patients with 7 or more decades of psoriasis (25.7% in the patients 61~70 years, 11.4% in those over 70 years; p=0.032) (Table 4). The mean age of the patient group with metabolic syndrome (52.54±13.09 years) was higher than that of the patients without metabolic syndrome (43.42±16.92 years) (p<0.005) (Table 5). Metabolic syndrome was observed in 34.3% of the psoriasis patients with a family history of psoriasis and in 65.7% of those without a family history of psoriasis (p<0.05) (Table 4). None of the mild-psoriasis patients had been unable to receive systemic treatment because of old age, a general poor condition or infection. The prevalence of metabolic syndrome was 97.1% in the cases of moderate to severe psoriasis, and it was higher than 2.9% in the mild psoriasis cases (p<0.05) (Table 4).
The multivariate logistic regression analysis also showed the same results, that age (p<0.01), a family history of psoriasis (p<0.05) and the severity of psoriasis (p<0.05) were the significant risk factors for metabolic syndrome in the patients with psoriasis (Table 6).
Framingham risk score and the need for modifying the serum lipid profiles
To evaluate the cardiovascular risk in the patients with psoriasis, the Framingham 10-year risk score was calculated for the 159 patients (80.7%) with psoriasis and who were aged 20 and older and who do not have heart disease or diabetes. Forty-five (22.8%), 79 (40.1%), 25 (12.7%) and 10 (5.1%) of the 159 patients with psoriasis exhibited a 10-year risk less than 1%, 1~10%, 10~20% and over 20%, respectively. Seventy-three (37%) patients with psoriasis had LDL levels higher than the target LDL level proposed by the ATP III guideline. Among the 73 patients with higher LDL levels, 50 (25.3%) were determined to need lifestyle changes and 23 (11.7%) needed drug therapy to achieve the proper LDL level (Table 7).
DISCUSSION
Psoriasis is one of the most common chronic inflammatory skin disorders, and it can be accompanied by arthritis, a low quality of life and depression1-3. Psoriasis is now considered a systemic inflammatory disease, with Th-1 cells, Th-17 cells and inflammatory cytokines contributing to its pathogenesis1-5. Inflammatory markers such as Th-1 cytokines (intracellular adhesion molecule-1, TNF-α) play a role not only in the pathogenesis of psoriasis, but also in the pathogenesis of metabolic syndrome, obesity, atherosclerosis and myocardial infarction5-7,15,16. In addition, the patients with psoriasis have elevated levels of C-reactive protein (CRP), which has been independently associated with an increased risk of cardiovascular disease17-19. Genetic investigations have demonstrated an association between psoriasis and the cardiovascular risk factors. The replicated genetic loci identified in psoriasis patients, such as CDKALI, have been associated with type 2 diabetes20. Apolipoprotein E-4 (APOE4) is a gene related to blood cholesterol levels, and it has been reported to be associated with psoriasis21. Furthermore, variations of the TNF inducible protein A20 (TNFAIP3) gene, which is known to be associated with psoriasis, have been shown to increase coronary artery disease22,23.
In fact, recent investigations have reported the possible association between psoriasis and cardiovascular disease and its risk factors. Several studies have reported a higher prevalence of smoking, diabetes and hypertension among the patients with psoriasis compared with that of the controls24-28. The level of lipids such as TG and LDL has been shown to be elevated in patients with psoriasis7,29. Furthermore, the prevalence of ischemic heart disease and peripheral arterial disease, as well as metabolic syndrome that affects the cardiovascular morbidity and mortality, was higher in patients with psoriasis as compared to that of the controls7,25,28,30-32.
However, there is no reported study about the association between psoriasis and cardiovascular disease and the risk factors for cardiovascular disease in Koreans. In this study, a higher prevalence of metabolic syndrome (p=0.021) and cardiovascular diseases (p=0.044) was observed among the patients with psoriasis as compared to that of the controls. The cardiovascular risk factors (smoking, obesity, hypertension, diabetes, and hyperlipidemia) were more prevalent in the patients with psoriasis than that in the controls. However, significant differences were only observed for hypertension (p=0.000) and hyperlipidemia (p=0.025). The χ2-test and multivariate logistic regression analysis also showed that age, a family history of psoriasis and the severity of psoriasis were the significant risk factors for metabolic syndrome in the psoriasis patients.
The severity of psoriasis was classified as described by Xiao et al31. This classification has several limitations. It is not able to represent the objective and numerical severity, and a few of the patients who were receiving systemic treatments may have belonged to the mild psoriasis classification rather than to a moderate to severe psoriasis classification. The psoriasis area and severity index (PASI), psoriasis global assessment (PGA) and the lattice system physician's global assessment (LS-PGA) have been commonly used to evaluate the response before and after treatments33. Yet these methods were inappropriate for measuring the severity of psoriasis in this cross-sectional study because the patients were already being treated at the time they enrolled in this study. Moreover, their medications, including cyclosporine, acitretin, etretinate and methotrexate, may have contributed to causing the cardiovascular risk factors. The adverse effects of cyclosporine are dyslipidemia and increased blood pressure9, and the adverse effect of acitretin and etretinate is dyslipidemia8. Methotrexate can increase the risk of atherogenesis by reducing the plasma folate levels and increasing the homocysteine levels10. Therefore, to assess the severity of psoriasis for determining the cardiovascular risk factors, the classification based on the medications in this cross-sectional study is thought to be appropriate.
To evaluate the absolute risk of major coronary events, we determined the Framingham 10-year risk score for the patients with psoriasis. The Framingham 10-year risk score, which is designed to estimate the 10-year risk for major coronary events, can be calculated by entering the gender, the smoking status, total cholesterol, HDL, the systolic blood pressure and any current high blood pressure medication that is being taken at the NCEP Internet site (http://hp2010.nhlbihin.net/atpiii/calculator.asp?usertype=prof). Furthermore, the U.S. Preventive Services Task Force34 proposed that aspirin should be used to prevent coronary heart diseases when the Framingham 5-year risk score is 3% or greater, or the 10-year risk score is 6% or greater, after consultation with the patients regarding the potential risks and benefits. In this study, a substantial portion of patients with psoriasis met the criteria for using aspirin, since 73 patients (37.0%) with psoriasis exhibited a 6% or greater Framingham 10-year risk.
It is well known that increased cholesterol levels are associated with the cardiovascular risk, and that lowering cholesterol can decrease this risk35. For this reason, the ATP III guideline14 recommends that the cholesterol levels should be regulated by focusing on LDL cholesterol, among the patients who are categorized as belonging to one of the four risk groups (high, moderate high, moderate and low) according to the cardiovascular risk factors and the Framingham risk score. The ATP III guideline established the LDL goal for each risk group and it recommended lifestyle changes and/or pharmacotherapy for maintaining proper LDL levels. This study showed that 73 patients (37%) with psoriasis needed lifestyle changes and/or drug therapy in order to decrease their LDL.
Although we confirmed the association between psoriasis and the cardiovascular risk factors, our study had several limitations. The observed association may be temporary because this study is a cross-sectional study. We could not determine whether this association was affected by the systemic inflammatory process of psoriasis, the side effects of medications (acitretin, cyclosporine, methotrexate and so on) or lifestyle factors such as depression and a low quality of life. Another limitation was that the sample size was not large enough to represent the general population. Recall and misclassification bias due to faulty recall and inaccurate diagnostic codes could not be completely excluded, although we tried to reduce these biases by interviewing the individuals in this study and reviewing the medical records. In addition, Stern36 commented that psoriasis is not a useful independent risk factor for cardiovascular disease because of the lack of objective criteria to classify the severity of psoriasis for the purposes of cardiovascular risk stratification, the low prevalence of severe psoriasis and the absence of a general population-based study. We hope that future prospective, randomized, controlled, population-based or multicenter studies will confirm the association and causality between psoriasis and cardiovascular risk factors.
On the basis of this study and similar studies, dermatologists and general practitioners should recognize the possible association between psoriasis and the cardiovascular risk factors. Although the benefits of screening and modifying the cardiovascular risk factors in patients with psoriasis have not yet been investigated, this study showed that a substantial portion of patients with psoriasis need prophylactic aspirin, lifestyle changes and/or lipid-lowering therapy according to their Framingham risk score and the ATP III guideline. Therefore, we suggest that clinicians pay attention to screen for and manage the cardiovascular risk factors when caring for patients with psoriasis.





 XML Download
XML Download