

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although vitiligo does not result in any restrictions on life expectancy or a patient's capacity to work, it can cause cosmetic disfigurement and may affect the psychological well being of patients1,2. The etiology of vitiligo remains unclear, but oxidative stress and the accumulation of free radicals have been proposed as important pathogenic mechanisms3-5. Increased malondialdehyde (MDA) levels are reported in the skin of patients with active vitiligo. Additionally, glutathione peroxidase (GPX) and superoxide dismutase (SOD) levels have been reported to be elevated in vitiligo patients3,6. The acquisition of tissue samples to test these levels is not easy, however. Thus, the majority of previous studies have used serum in which to measure oxidant or antioxidant levels. However, MDA levels in the serum are too low to be reliable. In the literature, it has been demonstrated that erythrocytes can reflect oxidative status more accurately than serum, as they are known to be prone to oxidative reactions7. In this study, we measured erythrocyte MDA, a well-known indicator of oxidative stress, to evaluate the level of reactive oxygen species (ROS).
Studies have shown that the level of catecholamines and their metabolites are increased in the skin lesions, plasma and urine of vitiligo patients8-10. It has also been reported that catecholamine-induced oxidative stress may involve free radical damage.
We previously reported that the dopamine-induced apoptosis of melanocytes might be a clue in understanding the pathogenesis of vitiligo. Interestingly, a study showed that thiol compounds, including N-acetylcysteine and glutathione (GSH), only block dopamine-induced melanocyte apoptosis11. In vitiligo patients, it has been reported that GPX levels are increased in tissue and reduced in erythrocytes. However, the levels of GSH in erythrocytes have not been well studied, even though GSH is quite effective against dopamine-induced melanocyte apoptosis. Therefore, we measured the GSH levels in erythrocytes. Furthermore, we analyzed the results according to the disease activity and each patient's habitual behaviors.
MATERIALS AND METHODS
Patients and controls
Fifty-three generalized vitiligo patients (28 women and 25 men, median age 32.1 years, range 17~58 years) were enrolled in this study. The patients had skin phototypes of III-V (Fitzpatrick classification), and the mean duration of disease in patients was 8.8 years. None of the patients had concomitant dermatological diseases, thyroid dysfunction, or any other autoimmune disease. Patients who had taken systemic steroids or been treated with systemic phototherapy within the past 2 months were excluded. The control group consisted of 65 healthy volunteers who denied systemic or dermatologic disease. The vitiligo and control groups were matched according to phototype, age, and sex.
Questionnaire
All the patients were instructed to answer a questionnaire. The questionnaire consisted of several questions (questions about disease activity and the patient's habitual behavior). Controls were asked whether they were smokers or not.
Preparation of samples
Blood was taken from the cubital median vein and placed into ethylenediaminetetraacetic acid (EDTA) tubes. The blood samples were centrifuged for 10 min at 1,000×g at 4℃, and the plasma was discarded. After the buffy coat was carefully removed, the remaining erythrocytes were diluted with 10 ml of isotonic NaCl solution. The resuspended erythrocytes were then centrifuged for 10 min at 1,000×g at 4℃, and the upper layer was removed. The erythrocytes were treated 3 times in this manner and then diluted 5 times in ice-cold water and vortexed. Samples were stored in multiple aliquots at -80℃ until analysis.
Analysis of lipid peroxidation
The MDA levels were determined using a Lipid Peroxidation Colorimetric Microplate Assay Kit (FR22, Oxford Biomedical Research Inc., Oxford, MI, USA). The samples were assayed in accordance with the manufacturer's instructions. The samples were mixed with diluted N-methyl-2-phenylindole, vortexed, and subsequently incubated for 60 min at 45℃. Thereafter, the samples were centrifuged for 15 min at 13,000×g. Absorbance was measured with an ELISA reader (Spectra Max Plus 384, Molecular Devices, Sunnyvale, CA, USA) at 586 nm. MDA concentrations were quantified via comparison with a standard curve ranging in concentration from 0 to 4µM and expressed per gram of total protein.
Glutathione determination
The GSH levels were determined using a Glutathione Assay kit (NWK-GSH01, Northwest Life Science Specialties, LLC, Vancouver, WA, USA). The samples were mixed with metaphosphoric acid, vortexed, and centrifuged for 5 min at 1,000×g. The supernatants were collected and assayed in accordance with the manufacturer's instructions. Supernatants were mixed with 5-5'-dithiobis (2-nitrobenzoic acid) (DTNB) and GSH reductase. Samples were incubated in darkness for 3~5 min and then the total GSH was quantified after kinetic spectrophotometric analysis at 408 nm using an ELISA reader (Spectra Max Plus 384, Molecular Devices). GSH concentrations were expressed per gram of total protein measured.
RESULTS
All the vitiligo patients were the generalized type. Table 1 shows subtypes of patients.
The mean MDA level was slightly higher in the vitiligo patients (297±44) compared to the healthy controls (289±47), but no significant statistical differences were noted. The mean GSH level of erythrocytes was significantly lower in the patient group than in the control group (patient, 465±145 vs. controls, 598±131, p=0.000) (Table 2). In the vitiligo patients, MDA levels did not differ according to disease activity (Table 3). However, the levels of GSH in active cases were consistently lower than the GSH levels in less active cases. These observed differences were not statistically significant, however.
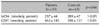
Table 4 shows the levels of MDA and GSH according to patients' habitual behaviors. While diet or drinking did not affect the level of MDA or GSH, smoking significantly lowered levels of GSH (smoking, 370±63 vs. non-smoking, 477±149, p=0.015).
All the subjects in the control group were non-smokers. In vitiligo, 47 of 53 patients were non-smokers. The levels of GSH were then compared between control non-smokers and vitiligo non-smokers. Interestingly, the mean level of GSH was also significantly lower in the patient group than in the control group (patients, 477±149 vs. controls, 598±131, p=0.008).
DISCUSSION
Although the pathogenesis of vitiligo remains to be elucidated, many possible causes have been proposed to explain the destruction of melanocytes, including neural and autoimmune disorders, oxidative stress, and an inherent defect theory. Among these, oxidative stress is a well-established trigger factor for melanocyte degeneration12.
Oxidative stress can be induced by increased ROS generation. ROS play an important role in cell signaling, but insufficient antioxidant protection or excess ROS production causes oxidative damage. ROS can then induce a cytotoxic effect in melanocytes via the induction of melanocyte apoptosis or an autoimmune response via the modification of melanocytic antigens13-16.
In this study we measured erythrocyte MDA, a well-known indicator of oxidative stress, as erythrocytes can reflect oxidative status more accurately than serum7. Indeed, studies have demonstrated that patients with Behcet's disease have higher levels of MDA in erythrocytes than in plasma17. Our results suggested that erythrocyte MDA levels were not altered in vitiligo patients regardless of disease activity. Previous studies have shown higher MDA levels in both serum and tissues in vitiligo patients compared to healthy controls3,4,6,8-10,15. Thus, these findings suggest that erythrocyte MDA levels are not closely correlated with the tissue levels of MDA in vitiligo patients. However, further study will be required.
We subsequently measured the levels of GSH in erythrocytes. We previously reported that GSH can prevent the dopamine (DA)-induced apoptosis of melanocytes and their signaling11. Among various antioxidants, only thiol-containing antioxidants such as N-acetylcysteine (NAC) or GSH showed protective capability.
MDA, an end product of lipid peroxidation, is a well-established indicator of oxidative stress. Even though erythrocyte MDA levels were found to be within the normal range in our study, previous studies have demonstrated higher MDA levels in lesions of vitiligo patients. Thus, it should be expected that antioxidant levels would be reduced in these lesions. In the relevant literature, catalase levels were found to be reduced in lesions of vitiligo patients3,6. Additionally, increased levels of GPX have been reported3. However, the levels of GSH have not been thoroughly studied. In one older report, the levels of erythrocyte GSH in vitiligo patients were reported to be normal. In another study conducted by Yildirim et al., erythrocyte GSH levels were significantly lower in vitiligo patients compared to controls; these findings were in agreement with our results18. From these findings, we could surmise that reduced erythrocytic or systemic GSH levels are a distinctive feature of vitiligo patients. In other words, it is reasonable to assert that GSH is systemically exhausted to neutralize free radicals. Thus, it can also be asserted that reduced erythrocytic GSH levels can be a marker for vitiligo.
We then compared MDA and GSH values among different groups sorted by disease activity. Neither MDA nor GSH levels differed depending on disease activity. Thus, the systemic or erythrocytic levels of GSH cannot be considered to be markers of recent activity of vitiligo lesions. However, the levels of GSH in more active cases were consistently lower compared to GSH levels in less active cases. These results must be confirmed with an increased number of patients. We then analyzed the effects of environmental factors such as smoking, diet, and alcohol intake. While there remains some controversy regarding the effects of diet and drinking on the oxidative system, smoking is a well-established factor related to increased free radical production19. Previous studies have reported that GPX and PON1 activity were significantly lower in smokers, while MDA levels were higher in smokers20. In the present study, erythrocyte MDA levels did not differ according to patients' habitual behaviors, but the GSH levels were found to be lower in smoking patients compared to non-smoking patients. In addition, the mean level of GSH was also significantly lower in non-smoking patients compared to non-smoking controls. It is difficult to say that smoking plays an important role in the pathogenesis of vitiligo. Yet these results do support our assumption that a reduction in erythrocytic or systemic antioxidants, rather than an increase of oxidants, is associated with various oxidative stress conditions. Other habitual behaviors, including vitamin or dietary supplement intake, vegetable or fruit intake, and alcohol drinking were not associated with any difference between the patients and controls.
In summary, erythrocyte GSH levels were significantly lower in the vitiligo patients compared to the controls. However, erythrocyte MDA levels did not differ between the 2 groups. Additionally, smoking dramatically reduced the erythrocyte levels of GSH.
In conclusion, we conclude that a reduced erythrocytic or systemic GSH level is a distinctive feature of vitiligo. Additionally, cigarette smoking is believed to increase this imbalance. Thus, smoking should be prohibited in vitiligo patients to prevent the possible aggravation of the condition.


 XML Download
XML Download