

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Proliferation of eccrine units without vascular proliferation in the dermis is a characteristic feature of an eccrine nevus. To date, about 20 cases of eccrine nevi have been reported in the medical literature. Recently, an unusual variant of an eccrine nevus, a coccygeal polypoid eccrine nevus (CPEN), has been suggested1. CPENs are congenital, asymptomatic, polypoid lesions occurring in the coccygeal region. In the present report, we present two cases of CPENs and summarize the features of CPENs.
CASE REPORT
Case 1
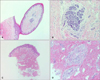
A 1-month-old boy was brought for evaluation of an asymptomatic skin lesion on the buttocks that was present since birth. He was in good physical health, and had no significant medical or family history. The physical examination revealed a 0.5 cm, flesh-colored papule on the midline of the coccyx (Fig. 1A). The lesion was not associated with any symptoms, such as hyperhidrosis, pain, or tenderness. A skin biopsy specimen, including the whole papule, showed a pedunculated configuration with an acanthotic epidermis and hyperkeratosis (Fig. 2A). In the center of the lesion, a distinct dermal proliferation of normal eccrine ducts and glands were present (Fig. 2B). There was no abnormal vascular proliferation noted, except for some vascular ectasia.
Case 2
An 8-year-old girl presented with an asymptomatic papule located on the coccygeal region that was present since birth. She had no significant medical or family history, and no evidence of systemic disease. Grossly, the lesion was a 0.5 cm skin-colored papule that was less pedunculated than the previous case (Fig. 1B). Microscopically, the lesion had an increased number of eccrine glands and ducts in the dermis without any other abnormalities, similar to case number 1 (Fig. 2C, D).
DISCUSSION
Eccrine nevi are rare, benign, cutaneous lesions characterized by an increase in the number or size of structurally normal eccrine coils2. There are about 20 cases reported in the medical literature with a variety of clinical manifestations. Eccrine nevi occur equally in males and females3, and are usually noted during childhood or adolescence, but are uncommon at birth. Although, most eccrine nevi present with localized hyperhidrosis, asymptomatic lesions have also been described, though uncommonly. In addition, these lesions are usually not associated with any cutaneous abnormalities. However, some unusual presentations, such as a hypopigmented patches and linear papules have been reported4,5. About one-half of the cases of eccrine nevi present on the upper extremities, and other locations, such as the back and trunk, have also been reported. The unusual location of sacral eccrine nevi has been reported in two cases; Mahdavy and Smoller6 reported an eccrine nevus in a 9-year-old girl presenting with an asymptomatic skin tag located in the coccygeal area. More recently, Oh et al.1 suggested that a CPEN should be considered as a distinct variant of the eccrine nevus, and presented the case of a 2-year-old girl. In our patients, small polypoid papules were located in the central coccygeal area, clinically identical to the previously reported cases. Therefore, the lesions can be regarded as CPENs. Although, the number of reports is limited, and more cases are necessary, the characteristics of the reported CPENs might be summarized as follows: congenital, asymptomatic, not associated with hyperhidrosis, and resembling a skin tag. A skin tag can be differentiated from a CPEN by the flattened epidermis, overlying loose collagen bundles, central fatty tissue, and the absence of abundant eccrine units7. In addition, the midlife occurrence of most skin tags is helpful in distinguishing the two entities. A mass on the sacrum can also be confused with a lumbosacral lipoma, which is a rare congenital anomaly. However, lumbosacral lipomas are always accompanied with spinal defects, such as spina bifida, and consist of mature fat tissue on histologic examination8. An eccrine angiomatous harmatoma (EAH) should also be considered in the differential diagnosis. Clinically, EAHs may present as papules or nodules on the extremities that are occasionally accompanied by hyperhidrosis and/or pain3. Histologically, EAHs are usually located in the deep dermis and contain increased eccrine units, as well as abundant capillary proliferation, which was not present in the cases reported herein9.
In summary, we have presented the unique manifestations of eccrine nevi in two patients, reviewed similar cases in the literature, and summarized the characteristics of CPENs. CPENs should be considered in the differential diagnosis of coccygeal papules occurring in children.

 XML Download
XML Download