

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lichen aureus is a rare type of chronic pigmented purpuric dermatosis. It is usually characterized by a single localized golden macule on an extremity1. Five cases of lichen aureus have been reported in the Korean literature2-6. However, a childhood case has not been previously reported. We herein report the first case of multiple lichen aureus in an 8-year-old Korean child.
CASE REPORT
An 8-year-old Korean girl presented with a single asymptomatic round brownish patch on the right arm and two similar shaped patches on the left leg. The lesion on the arm first appeared one year previously, and the lesions on the leg started to appear three months ago. There was a history of a right tibial fracture four months ago, and no other preceding trauma around the skin lesions. Routine laboratory tests during hospitalization for treatment of the fracture showed slightly elevated liver enzymes (AST: 58 IU/L, normal 0~40 IU/L; ALT: 111 IU/L, normal 0~40 IU/L), which were thought to reflect a non-alcoholic steatohepatitis due to obesity. No other significant health problems or family history of similar disorders were noted. Physical examination revealed multiple round patches of yellow or brown on the right upper arm and left leg (Fig. 1). No evidence of other skin diseases was noted on complete examination of the skin.
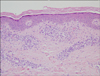
Histopathological examination of the left leg revealed a perivascular lymphocytic infiltration in the upper dermis with extravasation of red blood cells and mild exocytosis of lymphocytes in the epidermis (Fig. 2). Based on these clinical and histopathological features, the skin lesion was diagnosed as multiple lichen aureus.
The patient was treated with 0.1% methylprednisolone aceponate cream applied twice a day for four months. At the end of this time, the lesions were nearly completely resolved (Fig. 3).
DISCUSSION
Lichen aureus is an uncommon variant of pigmented purpuric dermatosis, which was first described by Marten7 in 1958. Most cases manifest as asymptomatic discrete or confluent golden to brownish lichenoid macules and papules that clinically resemble a bruise. The lesions usually persist unchanged for many years8,9. In a review of cases reported by Price et al.8, the average duration of lichen aureus is about 2.5 years (range, 1~10 years). Lichen aureus commonly occurs in young adults and the involved sites are most often on the lower legs.
Childhood lichen aureus has some distinctive characteristics. First, in general, it occurs less frequently than in adults10,11. Gelmetti et al.10 reported that only 17% of the total number of cases included children. Second, the disease in children is more self-limiting compared to the disease in adults10. Third, uncommon sites such as the trunk and arms are more frequently observed in children1,10. In children, Schamberg disease and lichen aureus are relatively common types of pigmented purpuric dermatosis; however, Majocchi's disease and eczematoid-like purpura of Doucas and Kapetanakis are very rare. To date, pigmented purpuric lichenoid dermatosis of Gougerot and Blum has not been reported in children.
The etiology of lichen aureus remains unknown but several mechanisms have been suggested including venous insufficiency12, infection13 and drugs14.
Histopathologically, lichen aureus differs from other purpuric pigmented dermatoses by variable exocytosis of lymphocytes, lichenoid infiltration of superficial dermis, and marked accumulation of hemosiderin-containing macrophages8. Many reports on the prognosis of lichen aureus have suggested that lichen aureus may potentially progress to mycosis fungoides with similar histologic findings and clonal populations of lymphocytes15. But a recent study shows that no progression to mycosis fungoides was observed in 23 patients with conventional lichen aureus16. Although a relationship between lichen aureus and mycosis fungoides is debatable, lichen aureus belongs to the expanding spectrum of clonal dermatoses17, and possible progression to mycosis fungoides cannot be ruled out. Therefore, patients with lichen aureus should have regular follow up and remain under close observation.
Lichen aureus is generally considered difficult to treat as topical corticosteroids are usually ineffective9,11. Recent case reports suggest several treatments for lichen aureus: psolaren-UVA therapy18, topical pimecrolimus19, and combination therapy with pentoxifylline and prostacyclin20 have elicited good patient responses.
Our patient had multiple lesions on the arm and leg, which was an uncommon presentation. Although the patient had trauma and underlying steatohepatitis, the correlation of these factors to the development of the lichen aureus is uncertain; indeed the first lichen aureus lesion developed before the trauma. Unlike previous cases, topical steroid treatment was effective in our patient.
To date, five cases of lichen aureus have been reported in the Korean literature2-6; however, none of the cases included a prepubertal child. In addition, we could find only two cases of Asian childhood lichen aureus in our review of the published English medical literature. Lichen aureus in children has a tendency to be overlooked because it is so rare and presents with variable clinical features. It can be confused with contact dermatitis, stasis dermatitis, purpura, and other types of pigmented purpuric dermatoses. Histopathological characteristics and their incidence can help to make the exact diagnosis. Therefore, lichen aureus should be considered in the differential diagnosis of skin lesions that appear to be a simple bruise in children and need to be differentiated.


 XML Download
XML Download