

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hydroxyurea is a cytostatic agent that is currently the treatment of choice for various myeloproliferative diseases, such as chronic myelogenous leukemia, polycythemia vera, and essential thrombocytosis1. It acts during cellular replication and inhibits DNA synthesis by blocking ribonucleotide reductase2.
The most common adverse effects of hydroxyurea include mild fatigue, headache, nausea, vomiting, diarrhea, and fever. Severe side effects are rare and appear to be linked to long-term administration3. Adverse cutaneous effects include xerosis, diffuse hyperpigmentation, nail discoloration, alopecia, scaling, skin atrophy, skin tumors, lichen planus-like eruptions, and dermatomyositis-like eruptions1,3. In addition, a rare cutaneous manifestation, leg ulceration, has been reported in a few studies1. We report a case of a 75-year-old woman with essential thrombocytosis who developed painful leg ulcers, xerosis, and nail discoloration after hydroxyurea therapy.
CASE REPORT
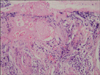
A 75-year-old woman presented with leg ulcers and xerosis. She had been diagnosed with essential thrombocytosis and had been receiving hydroxyurea therapy, 2 g/day, for 4 years. Scaly, hyperkeratotic patches and fissures were present on both of her heels. After she had rubbed her right heel, an erythematous ulcerative patch had developed (Fig. 1). The skin lesion on the right heel had progressed to become a deeper, severely painful, hemorrhagic ulcer; a similar lesion soon developed on her left heel (Fig. 1). Complete blood cell count revealed a hemoglobin of 9.2 g/dl, and a platelet count of 788×103/µl. No bacteria was found on Gram stains from the right heel wound. Bacterial and fungal cultures revealed no growth. Histologic examination of the specimen taken from the right heel showed mixed inflammatory cell infiltration around the dermal vessels, along with disruption of the epidermis (Fig. 2).
Although no definitive diagnosis was made, the patient started conservative treatment with antibiotics, analgesics, and occlusive dressings. However, the lesions did not improve during 5 weeks of treatment, and a new, painful ulcerative skin lesion developed on the left malleolus (Fig. 3). Longitudinal linear streaks and hyperpigmentation were noted in both the toenails and fingernails. The ulcers on both heels and the right malleolus became enlarged and more painful.
We began to suspect the side effects of long-term hydroxyurea administration, and we therefore discontinued the drug. The ulcerative skin lesions improved within 3 weeks (Fig. 4). We subsequently diagnosed the patient with hydroxyurea-induced leg ulcers. The cutaneous ulcers and xerosis completely disappeared within 2 months without recurrence, and the nail hyperpigmentation improved gradually.
DISCUSSION
Hydroxyurea is a cytostatic agent that serves as the drug of choice in the treatment of myeloproliferative disease. Because it acts during cellular replication (S phase) by blocking ribonucleotide reductase, the conversion of ribonucleotide to deoxynucleotide is inhibited1,2. Adverse cutaneous effects associated with hydroxyurea have been occasionally described in the literature. Xerosis, diffuse hyperpigmentation, nail discoloration, alopecia, scaling, skin atrophy, skin tumors, lichen planus-like eruptions, and dermatomyositis-like eruptions represent the majority of adverse effects1,3. In addition, leg ulcers have been noted in association with long-term hydroxyurea administration. Nine percent of patients taking hydroxyurea medication develop this complication4.
There is still controversy concerning the origin of the cutaneous ulcers-whether they are disease-related or treatment-related. Myeloproliferative disorders can impair cutaneous microcirculation. One theory says that the hyperviscosity resulting from blood dyscrasias may itself be a further risk factor for leg ulceration5,6. However, ulcerative skin lesions appear after the myeloproliferative disorder is well controlled with hydroxyurea. Furthermore, the lesions disappear after hydroxyurea is discontinued. Paradoxically, the ulcers have been shown to improve when the blood dyscrasia recurs1. So, in our opinion, hyperviscosity can be ruled out as a major contributor to ulcer formation.
Hydroxyurea treatment induces ulcerative skin lesion formation secondary to direct cytologic damage. Because hydroxyurea kills proliferating cells during the synthesis phase of the cell cycle, keratinocyte and collagen fiber synthesis could be impaired7. This hydroxyurea-induced compromise of skin formation could cause ulceration if followed by minor trauma, like rubbing in the present case8. A recent study showed that hydroxyurea can lead to increases in red blood cell volume and a reduction in red blood cell susceptibility to deformation. Therefore, it may cause impaired microcirculation and cutaneous anoxia, which then lead to ulcerative skin lesions and severe pain9,10. Bader et al11 proposed some criteria to help in diagnosis and differentiation. First, the duration of treatment should be at least 1 year, and the dose of hydroxyurea should be at least 1 g/day. Most ulcers are found on the malleoli (77%) or in neighboring regions (e.g. the Achilles tendon). Healing is slow (1~9 months) but spontaneous in 85% of patients after discontinuation of hydroxyurea therapy, and when hydroxyurea therapy is resumed, the ulcers do not resolve spontaneously and are difficult to treat. Ulcers are small, and size seems to be correlated with the hydroxyurea dose.
The treatment of choice for hydroxyurea-induced leg ulcers is discontinuation of the drug. Other reported therapies including topical granulocyte macrophage colonystimulating factor (GM-CSF), recombinant human erythropoietin (r-HuEPO), or bilayered bioengineered skin substitute12. In one report, a patient was successfully treated with prostaglandin E1 and pentoxifylline while hydroxyurea was continued13. In the present case, the cutaneous ulcers and xerosis completely healed within 2 months without recurrence, and nail hyperpigmentation gradually improved after hydroxyurea was discontinued.
The present case shows that long-term administration of hydroxyurea can result in ulcerative skin lesions of the lower legs, like other cases that have been reported in Korea14,15. Because hydroxyurea has long been the treatment of choice for myeloproliferative disorders, the possibility that cutaneous side effects will occur in patients treated with hydroxyurea always exists. Leg ulcers represent 9% of these side effects. Therefore, physicians should not overlook this adverse effect and must perform careful history-taking. In addition, because discontinuation of hydroxyurea can cause a hematologic crisis, a hematooncologist should be consulted, and periodic laboratory examinations should be performed.



 XML Download
XML Download