

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neonatal lupus erythematosus (NLE) is an uncommon immune-mediated disease that is associated with transplacental transfer of maternal IgG autoantibodies. Approximately half of the affected neonates have congenital heart block (CHB). Cutaneous lesions occur in approximately 50% of these patients and they typically consist of transient, erythematous, annular, and scaling plaques in sun-exposed areas, and these lesions resemble subacute cutaneous lupus erythematosus both clinically and histologically. Skin lesions and heart block are seen simultaneously in less than 10% of the patients with NLE1. Transient hepatitis, anemia, and thrombocytopenia can also occur2-10.
There have been 18 case reports of NLE in the Korean literature, including 7 case reports in the dermatological field of which 3 cases showed anemia and hepatitis (Table 1)6-22. We describe herein another case of NLE that displayed transient anemia and hepatitis. In addition, we review the cases of NLE in the Korean literature.
CASE REPORT
A 4-week-old, full-term, female infant, whose birth and life had been otherwise gone well, was brought to the dermatological clinic with a 3-week history of erythematous and annular plaques on the face and lower extremities (Fig. 1). The physical examination revealed no other abnormalities.
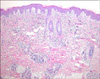
A biopsy from the face showed slight keratin plugging of the hair follicles, focal hydropic degeneration of the basal layer in the epidermis and a patchy perivascular, periadnexal, and interstitial infiltrate of lymphohistiocytes in the whole dermis (Fig. 2).
The patient's antinuclear antibody (ANA) titer was 1:320 with a homogeneous pattern. The tests for anti-SSA/Ro antibody and anti-SSB/La antibody were positive. The results of the electrocardiogram (ECG) were normal, but mild anemia (hemoglobin 8.3 g/dl) and hepatitis (AST/ALT 75/112 IU/L) were present.
The 25-year-old mother had no history of connective tissue disease and she was asymptomatic. The serological studies of the mother showed the presence of anti-SSA/Ro antibody and anti-SSB/La antibody. The mother's ANA titer was 1:640 with a homogeneous pattern.
The patient received topical corticosteroid and the skin lesions completely disappeared 6 months later without any residual atrophy or hyperpigmentation. At that time, the infant had an ANA titer less than 1:40; both anti-SSA/Ro antibody and anti-SSB/La antibody became negative and the complete blood cell count and liver function tests were normal.
DISCUSSION
NLE is an uncommon autoimmune disease that is associated with the transplacental transfer of maternal IgG autoantibodies. Only 1% of neonates develop NLE if the mother has autoantibodies. If an anti-SSA/Ro positive mother has one child with NLE, then 25% of the future siblings will also be affected. In 95% of the cases, the autoantibody is anti-SSA/Ro, but it can be anti-SSB/La or anti-U1RNP1. Any of these autoantibodies can be found alone or in combinations. Only cutaneous disease has been reported for the cases where only anti-U1RNP antibodies are found20,23. There are even reports of histological documented cases of NLE where none of the above-listed antibodies were found24. This finding suggests that antibodies other than anti-SSA/Ro, anti-SSB/La, or anti-U1RNP can be involved in some cases, and perhaps by some factor or cofactor that has yet to be determined.
The major clinical manifestations of NLE are cardiac problems, including CHB, and cutaneous lesions1. CHB can result in congestive heart failure and the subsequent placement of a pacemaker. In one investigation, 57% of these patients eventually required a pacemaker25. CHB is associated with a 20~30% mortality rate during the neonatal period. Deaths may also occur later in life as a result of the failure of the pacemaker. There have been five CHB patients reported in the Korean literature. Among them, three showed a spontaneous remission, one needed pacemaker insertion and one passed away. On the other hand, the cutaneous lesions of NLE consist of transient nonscarring erythematous annular plaques with a predilection for the periorbital and photodistributed areas. These lesions generally appear within the first 2 months of life and they resolve within 4 to 6 months when the maternal antibodies disappear. In rare cases, remnant telangiectasias can occur at the previously affected sites26.
Hepatic and hematologic abnormalities are observed in approximately 10% of the infants with NLE10. Hepatitis, hyperbilirubinemia, liver failure, thrombocytopenia, and anemia can occur2-10. The prognosis of a NLE patient with liver failure is poor, whereas for the NLE patients with other manifestations, the prognosis is good with transient involvement and spontaneous resolution. In the Korean literature, anemia occurred in 5 cases, thrombocytopenia occurred in 2 cases, and hepatitis occurred in 4 cases. Only 3 cases showed anemia and hepatitis simultaneously. Our patient showed typical cutaneous lesions, transient hepatitis, and anemia without cardiac involvement.
The association of NLE with maternal autoantibodies is a strong indicator of the importance of autoantibodies for determining the pathogenesis of NLE27. In patients with NLE, the autoantibodies are maternal in origin and they disappear by 6 months of age. These autoantibodies have the capacity to cause direct injury to the skin and the cardiac, hepatobiliary and hematologic system28. The disappearance of autoantibodies parallels the disappearance of the cutaneous, hematologic, and hepatic abnormalities. However, in patients suffering with CHB, immunodeposits of autoantibodies may result in fibrosis and calcification in and around the artrioventricular node, which can lead to permanent conduction defects.
The diagnosis of NLE is generally based on the clinical findings when there are maternal and/or neonatal autoantibodies present. Determining the titers of ANA and anti-SSA/Ro, anti-SSB/La, and anti-U1RNP antibodies is recommended for making the diagnosis. Liver function tests and a complete blood cell count should also be done. All the patients suspected of having NLE should undergo a thorough cardiac examination.
Spontaneous resolution is the natural course of the cutaneous lesions. However, management of the skin lesions of NLE requires avoiding sun light and using sunscreen and low-potency topical corticosteroids to hasten resolution. Treatment of the heart block is not necessary unless cardiac failure is evident.
Many (40%) of the affected infants' mothers are asymptomatic. They might have Sjögren's syndrome, systemic lupus erythematosus, rheumatoid arthritis, overlap syndrome or even leukocytoclastic vasculitis. Although the outlook of these mothers appears to be generally good, there is the possibility of developing serious autoimmune disease29. Thus, close observation is necessary for the mothers of infants with NLE.
In conclusion, we describe here an additional case of NLE that displayed transient anemia and hepatitis.


 XML Download
XML Download