

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Eccrine angiomatous hamartomas (EAH) are benign cutaneous hamartomas, often localized in the distal extremities of children or young adults. They are usually asymptomatic, although they may be painful and hyperhidrotic1. EAHs are composed of enlarged eccrine sweat glands intimately associated with small blood vessels located in the middle to deep dermis. Five cases of EAH have been reported in the Korean literature. However, EAH associated with verrucous hemangioma has not been reported in the Korean literature. We report an interesting case of EAH associated with verrucous hemangioma.
CASE REPORT
A 47-year-old Korean woman presented to a dermatology clinic with a skin lesion on the right sole, which had been present since birth. It had been increasing in size over a 1-month period after the patient had sustained trauma. The patient also noted pain and focal hyperhidrosis. Her personal and family histories were unremarkable. Physical examination revealed an erythematous keratotic plaque overlying a 5-cm sized, bluish, ill-defined plaque on the right sole (Fig. 1).
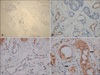
An incisional biopsy showed that the lesion had marked verrucous changes, including hyperkeratosis, papillomatosis, and irregular acanthosis in the epidermis, numerous dilated capillaries, and some congested vessels in the papillary dermis (Fig. 2, 3A). A nodular proliferation of eccrine glands was intimately admixed with numerous small vessels in the middle to deep dermis (Fig. 2, 3B). The epithelial cells of the eccrine glands were positive for CEA (Fig. 4), and the endothelial cells of numerous dilated capillaries were positive for CD31 and GLUT-1 (Fig. 5).
On the basis of these histological findings, we made a diagnosis of EAH associated with verrucous hemangioma.
DISCUSSION
EAHs are vascular and eccrine malformations, often localized in the distal extremities. They may be congenital or may appear later in childhood1. Clinically, they present as solitary papules or, rarely, in multiple distribution. They may be red, yellow, or brown in color. They are usually asymptomatic, although they may be painful and hyperhidrotic. Histologically, EAHs show enlarged eccrine sweat glands in the middle and lower dermis, intimately associated with thin-walled, aggregated vessels. The secretory portions of the eccrine glands are positive for S-100, CEA, and EMA.
EAHs have been reported in combination with other vascular tumors in a few cases. One had elements of an arterio-venous malformation, in which vessels showed uneven proliferation of intima and muscular walls2. Another was associated with a spindle cell hemangioma3. It contained vascular components consisting of dilated vessels intermixed with spindle cells3. A case of EAH with overlying verrucous hemangioma-like features has been described. However, the vessels were negative for GLUT-1, supporting the impression of hamartoma4.
Epidermal proliferation with verrucous features has been found in rare cases of EAH5,6. However, in these cases, other findings of verrucous hemangiomas, such as dilated capillaries and congested vessels in the papillary dermis, have not been observed.
Verrucous hemangiomas are rare vascular malformations, first described by Imperial and Helwig7 in 1967. They are a structural variant of capillary or cavernous hemangiomas, in which reactive epidermal changes develop secondarily. They usually involve the lower extremities, and their onset is near the time of birth or, less frequently, in early infancy7. The clinical appearance of a verrucous hemangioma changes with time7. Initially, it is a unilateral and circumscribed grouped of warty papules or plaques, bluish red in color. Later, it develops into a hyperkeratotic hemangiomatous papule in a linear or serpiginous configuration. Finally, the lesion becomes verrucous as a result of trauma and secondary infection. Histologically, verrucous hemangiomas appear initially as capillary hemangiomas concentrated in the dermis, and they adopt a verruciform pattern with papillomatosis, irregular acanthosis, and cavernous or mixed hemangiomas in the dermis and subcutaneous tissue8. Immunostaining shows focal glucose transporter-1 protein (GLUT-1) endothelial positivity9.
Our case showed marked verrucous changes in the epidermis and numerous dilated capillaries in the papillary dermis. There was positive GLUT-1 immunostaining in the endothelial cells of numerous dilated capillaries. According to these findings, a diagnosis of verrucous hemangioma was favored over hamartomatous change or angiokeratoma circumscriptum, which is an acquired dermatosis histologically characterized by dilatation of the vessels of the papillary dermis, without involvement of the deep dermis or hypodermis, and with hyperkeratosis10.
To our knowledge, no investigators have reported the coexistence of EAH and verrucous hemangioma with GLUT-1 positivity. Therefore, we report an interesting case in which these two entities co-exist.




 XML Download
XML Download