

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Steatocystoma multiplex is a hamartomatous malformation of the pilosebaceous duct junction1. It is a distinct clinical condition that's characterized by numerous small, skin-colored or yellowish, cutaneous cysts2. The lesions typically appear in childhood or early adulthood, but in some patients the lesions have developed late in life3,4. The cysts are located principally on the axillae, groin, trunk, scrotum and proximal extremities and they are rarely localized to the face and scalp3-6. Steatocystoma multiplex located on the face and scalp has been divided into three types3-6: 1) a facial papular variant type5, 2) sebocystomatosis6 and 3) cysts located exclusively on the scalp3,4.
We report herein a rare variant of steatocystoma multiplex that developed in an elderly woman and this condition was limited to the scalp.
CASE REPORT
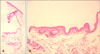
A 63-year-old woman visited our clinic because of papules on her scalp, and these papules had been slowly growing over a period of 2 years. On physical examination, several smooth-surfaced, round, yellowish papules were located on the left temporal part of the scalp. The diameter of the lesions varied from 3~5 mm (Fig. 1). No other lesions were observed on the extremities, trunk or face. The patient's past and family histories were non-contributory and the results of routine laboratory findings were within normal limits. A punch biopsy was performed to differentiate an eruptive vellus hair cyst, xanthomatosis and steatocystoma multiplex from other dermatologic conditions. When the surface skin of the yellowish papule was disrupted, a homogenous, creamy, odorless, yellowish material was expressed. The histologic examination showed an empty cyst with a folded wall in the mid-dermis. The wall of the cyst was composed of several layers of stratified squamous epithelium without a granular layer (Fig. 2A). Flattened sebaceous gland lobules were lying close to the cyst wall (Fig. 2B): these findings were consistent with steatocystoma. Some of the lesions were surgically excised, but the patient declined further treatment.
DISCUSSION
Steatocystoma multiplex is an uncommon disorder that's characterized by multiple soft, movable, small, cystic nodules. The diameter of lesions typically varies from 0.2~2 cm, but the nodules may be larger. The overlying epidermis is usually normal with no central punctum present. The lesions are typically located on the upper trunk, neck, axillae, scrotum and proximal extremities2. There may also be cases where there are scattered lesions on the scalp or face; however, it is very rare that the lesions are limited to the scalp (Table 1)3,4,7-12.
The pathogenesis of these lesions has been extensively studied. Steatocystomas were initially thought to be sebaceous or retention cysts13. In 1964, Kligman and Kirschbaum14 included these as a variant of dermoid cysts because of the presence of both hair shafts and sebaceous lobules. Steatocystomas are now recognized as a nevoid or hamartomatous malformation of the pilosebaceous junction1.
Steatocystoma multiplex is usually hereditary and it is inheirited as an autosomal dominant trait. However, it is nonhereditary for cases that the lesions are mainly limited to the scalp. The differences between typical steatocystoma multiplex and that limited to the scalp are presented in Table 2. In 1996, Lee et al6 reported on a case of sebocystomatosis that displayed multiple lesions of steatocystoma multiplex confined only to the forehead and frontal scalp together with congenital alopecia, and this was considered as a clinical variant of steatocystoma multiplex. Steatocystoma simplex, which is rarely found on the scalp, was first described as a distinct entity by Brownstein15 in 1982. It is similar to our case for the pathogenesis, the genetic propensity and the prognosis; however, steatocystoma simplex has a solitary nature (Table 2)15-18. Lim et al12 presented a patient with eruptive steatocystoma multiplex on the scalp. It was different from our case in that the lesions had appeared abruptly within a short period of time and the cysts showed an ovoid dilated cyst wall on histological study. Our case is educationally unique for the following points: (1) the presence of several cysts limited to the scalp, (2) no family history of similar lesions, (3) a late onset for the condition and (4) no congenital alopecia.
The causative factors of steatocystoma multiplex remain unclear, yet Setoyama et al11 suggested that trauma, infection or immunological events might be responsible. Some authors have reported that steatocystoma multiplex has been associated with ichthyosis and koilonychia, pachyonychia congenita, acrokeratosis verruciformis of Hopf, hypertrophic lichen planus, hypohidrosis, hypothyroidism, hidradenitis suppurativa and hypotrichosis4,18,19. For steatocystoma multiplex limited to the scalp, there have been no reports about specific causative factors and the relationship with other disorder, as was the case for our patient3,4,7-12.
The clinical differential diagnosis of steatocystoma multiplex includes multiple epidermoid cysts, eruptive vellus hair cyst, neurofibromatosis, lipomas and xanthomatosis. A skin biopsy specimen from a representative lesion is diagnostic. The characteristic histopathologic finding of the disease is the presence of flattened sebaceous lobules close to the cystic wall. The wall is composed of stratified, squamous epithelium without a granular layer. There are acellular eosinophilic cuticles on the luminal side of the cyst wall and keratin, oil or hairs in the lumen2.
Treatment of steatocystoma multiplex is largely symptomatic. Removal of these lesions can be successfully achieved with simple excision or drainage of the cyst materials. Inflamed lesions have been reported to respond to intralesional steroid injections, carbon dioxide laser, oral retinoids or cryotherapy2. The lesions are typically asymptomatic, but they are often cosmetically disconcerting. Our patient declined further treatment after the diagnosis was made.
We report here on a rare case of steatocystoma multiplex that sporadically developed in an elderly woman and the condition was limited to the scalp.



 XML Download
XML Download