

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acanthosis nigricans (AN) is characterized by symmetric, velvety, gray-brown hypertrophied plaques most commonly on the axillae and neck1. Confluent and reticulated papillomatosis (CRP) is manifested clinically by papules in the mid-chest that coalesce in the midline, and are arranged in a reticulated pattern peripherally2. Even though there are some reports of CRP without papillomatosis, AN and CRP characteristically have papillomatosis, irregular acanthosis, and orthohyperkeratosis on the histologic exams1234. Both diseases are known to be related to endocrinopathies such as diabetes mellitus(DM), an insulin resistant state and obesity with unknown mechanisms1.
CASE REPORT
Case 1
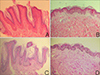
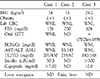
A 40-year-old female patient presented with a 10-year history of asymptomatic, symmetric, slowly progressive, skin eruptions. The eruption consisted of reticulated, brownish patches on the trunk and grayish, velvety plaques on both axillary folds (Fig. 1A). She denied any family history or personal history of similar eruptions or diabetes. However, she was on the antihypertensive medication. The results of physical, laboratory and histopathologic examinations of the patient and two other similar patients are summarized in Table 1. Based on the physical and laboratory test results, she was diagnosed as having metabolic syndrome by WHO diagnostic criteria. Skin biopsy specimens were obtained from the trunk and axillae. The biopsy specimen from the trunk revealed findings such as mild hyperkeratosis and papillomatosis which are compatible with CRP, and the specimen from the axillae showed hyperkeratosis, papillomatosis and finger-like upward projection of dermal papillae which are consistent with AN (Fig. 2). Because oral minocycline was not available in our clinic, she received oral acitretin 20 mg daily. Both axillary and trunk lesions were slightly improved after 6 weeks (Fig. 1B).
Case 2
A 16-year-old male patient presented with a 5-year history of asymptomatic, symmetric, slowly progressive skin eruptions (Fig. 1C, D). There was no family history or other history of similar eruptions or diabetes. The eruption consisted of reticulated, brownish patches on the trunk and both popliteal area, and grayish, velvety plaques on both axillary folds. The patient was diagnosed with a fatty liver 4 years ago. Skin biopsy specimens were obtained from the trunk and axillae. The results were similar to those of case 1. Because he had a fatty liver, he had been treated with 0.025% topical tretinoin ointment for 5 weeks. However, he was follow-up lossed. He revisited one year later and has since received systemic acitretin 20 mg a day for 2 months. No definite improvement has been observed up to now.
Case 3
A 14-year-old female patient presented with a 3-year history of asymptomatic, symmetric, slowly progressive, skin eruptions (Fig. 1E, F). The eruptions were composed of reticulated, brownish patches on the central area of the trunk, and grayish, velvety plaques on the nuchal area. The patient complained about recent irregular menstruation. She had undergone endocrinologic evaluation. There were no abnormal findings but oral GTT was positive in the endocrinologic evaluation. Skin biopsy specimens were obtained from the trunk and axillae. The results were similar to those in case 1. She was treated with oral isotretinoin 200 mg daily with 12% lactic acid lotion for 3 months. During 3 months, no remarkable improvement has been observed. Because of refusal to receive long-term oral medication, she stopped treatment without any improvement.
DISCUSSION
Although CRP and AN are associated with obesity, they are distinct entities with different clinical features2. However, a close relationship between the two is suggested by similar predisposing characteristics including young age, obese, dark-skinned persons and parallel response to weight reduction or etretinate therapy56. A pathogenetic link between the two conditions is suggested by insulin resistance and consequent hyperinsulinemia. High levels of circulating insulin have mitogenic and antiapoptotic activities on keratinocytes through activation of the tyrosine kinase (TK) receptor superfamily7. These activities may provide an explanation for the epidermal proliferation and papillomatosis observed in the above patients.
The patient in case 1 had the metabolic syndrome. The case 2 and case 3 patients had DM. Both disorders are known to be associated with insulin resistance. The presence of underlying endocrinopathies may explain the concurrent CRP and AN in our patients. There have been only two prior reports of concurrent CRP and AN reported in the medical literature56. However the coexistence of the two diseases is not rare. Rather, it is neglected. Even though these two diseases are now accepted as different ones, they still share common pathogenetic and histologic aspects. Thus, in order to improve our understanding of the pathogenic mechanisms underlying CRP and AN, and their association with obesity, further concern and study are received.

 XML Download
XML Download