

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The introduction of Mohs micrographic surgery minimized the loss of normal tissue while also enabling complete tumor resection. Thenceforth, Mohs micrographic surgery was used for various cutaneous neoplasms, and it was reported as the most efficient treatment method with regard to the recurrence rates and aesthetic aspects, relative to those of the various other methods that were being applied before. So far, a single-bladed scalpel that can be used for removing common malignant skin lesions has been used. The double-bladed scalpel, with its improved ability to excise uniform strips of tissue, was originally created to harvest donor strips for hair transplantation2. We describe a modified vertical method of Mohs micrographic surgery using the double-bladed scalpel, enabling unskilled surgeons to increase intraoperative efficiency.
CASE REPORT
A 58-year-old man presented with a 1-year history of a black mass measuring 2.0×0.5 cm on the right nasolabial fold. No pain, tenderness or itching was associated with the lesion which was pathologically diagnosed by biopsy as basal cell carcinoma.
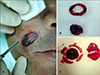
Basal cell carcinoma on the right nasolabial fold was completely removed with two stages of Mohs micrographic surgery. Similar to the routine method, incision is performed with a double-bladed scalpel using 11th blade after determining 2 mm safety margin (Fig. 1A). Vertical excision is done with the outer blade of the scalpel by following the excision width. At this time, two important points are 1) an 11th blade is generally used because it enables the surgeon to turn along the curving area easier than any other blade such as the 15th or 10th blade. 2) metal-spacers can control the excision width space as much as 1.5~2.0 mm. For instance, a 1.5 mm excision width is preferred when cancer occurs on the forehead because of the hardness of the forehead tissue. When the tissue is soft like those of the cheek, we use a 2.0 mm excision width. When the incision is sufficient to reach the subcutaneous fat layer, then the basal area is cut with a single-11th bladed scalpel, which divides the area into two sections (the margin and the main tumor) (Fig. 1B). Between these two sections, the direction of the margin strip must be marked and the margin strip must be subdivided into four segments. Then place the lateral side facing upwards and cut the basal segment from the main tumor so that the basal surface should also face upwards (Fig. 1C). The tissue is transferred to a Cryostat chuck with the lateral side up and being compressed. A few drops of OCT (Optimal Cutting Temperature) are placed over in such way that the edges and the depth are frozen at the same plane. The processes after this are identical as the routine Moh's technique. There were no tumor cells. The final surgical defects measured 2.5×1.5 cm. The tumor defect was covered by direct closure. The final shape and texture were satisfactory. No local recurrence or regional metastasis occurred for the following 2 years.
DISCUSSION
The double-bladed scalpel consists of a handle, blade holder and metal-spacers, as is shown on Fig. 2; this instrument can hold two blades and the distance between the two blades can be adjusted. This device was described in 1977 by Coiffman3, and it was originally developed for harvesting strip grafts from the scalp for hair transplantation. Up to 16 parallel blades have been placed on a single knife for this purpose4. The double-bladed scalpel has been employed for scar removal5, staged excision of lentigo maligna melanoma with permanent vertical section margin control6 and excision of small basal cell carcinoma78.
To get full analysis of the margin of tumor, the surgeon must perform some type of "en face" resection of the margin, meaning that the entire peripheral margin must be excised and examined. For standard surgical approaches, this usually implies taking a 1 mm rim of tissue cut at 90 degrees to the tissue and sending it in quadrants to pathology for frozen section analysis. Importantly, the thinner the rim of tissue, the less chance there is for a false-negative analysis occur. There have been recent reports of double bladed scalpels that are designed specifically for this purpose8. The use of this device in Mohs micrographic surgery of basal cell carcinoma has not previously been reported. We used a modified vertical method of Mohs micrographic surgery using the double-bladed scalpel, allowing to achieve a margin with uniform and even thickness.
Kopke et al9 classifies Mohs micrographic surgery into three categories: conventional method, marginal strip method and munich method.
While not necessary for the majority of routine Mohs cases, utilization of the double-bladed scalpel may be time-saving, especially when used for peripheral margin control. Moossavi M et al2 suggested the most important advantage of the double-bladed scalpel over the single blade is that it improves the ability of the surgeon to harvest uniform strips of tissue. Operator error is therefore reduced, since a precise tissue margin may be removed around any given lesion. The uniform strips are more easily processed for frozen section evaluation. The double bladed knife may lose the traditional beveling technique of Mohs micrographic excision, since the double-bladed scalpel is typically held perpendicular to the skin. Nevertheless, an experienced Mohs technician should be able to manipulate the tissue for sectioning so that the epidermal edge is visible pathologically. The use of the double-bladed scalpel in Mohs micrographic surgery for peripheral margin control of tumors increases intraoperative efficiency and allows for conservation of normal tissue. This available tool would be useful to unskilled surgeons operating on tumors requiring accurate peripheral margin control.
The advantages of this method are: 1) a margin with a uniform, even thickness can be gained, 2) due to the even thickness, the frozen section could be easily and precisely cut, requiring fewer tissue sections, 3) false negative results could be decreased, and 4) the operation time could also be decreased.

 XML Download
XML Download