

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nuchal-type fibroma is a rare, tumor-like proliferation originally described by Enzinger and Weiss1. One case was also reported in Korean dermatologic literature2. This process chiefly occurs in the dorsocervical area of adult patients, but may arise elsewhere in the subcutis. Affected patients' ages mainly ranged from 25 and 60 years. This lesion may be seen as a firm fibrofatty mass, and it consists of hypocellular dense bundles of collagen with interspersed fat tissue, nerve fiber, etc3. In early stage, nuchal-type fibromas were always reported on the posterior neck, therefore the term "nuchal fibroma" was picked up by authors. But, the term "nuchal-type fibroma" was proposed as the extranuchal lesions were also described3. Nuchal-type fibromas in extranuchal locations are often called extranuchal nuchal-type fibroma4. Nuchal-type fibroma in extranuchal locations most often involved the back or scapular region, shoulder, and face. These lesions are morphologically indistinguishable from the lesions involving the nuchal region. We report an adult with nuchal-type fibroma, which was located in coccyx area.
CASE REPORT
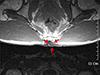
A 29-year-old man without any particular medical history presented to our institution with a 6-year history of asymptomatic lump on the coccyx area. The patient complained that it had been gradually growing. On physical examination, the lesion was 3 × 4 cm sized, not tender, subcutaneous mass on the left side of coccyx area (Fig. 1). There were no other specific physical and laboratory findings. MRI scans revealed a relatively ill-defined lesion on subcutaneous fat layer of posterior to coccyx. This lesion appeared low signal intensity on both T1 and T2-weighted images, and measured 4.0 × 3.6 × 1.7 cm . It was attached to, but had not extended into, the coccyx (Fig. 2).
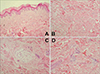
For further diagnosis and treatment, we performed total excision. Grossly, the mass showed unencapsulated, homogenous whitish fibrotic appearance. It was poorly demarcated, and attached somewhat to surrounding tissue. Histopathologic examination of this mass revealed sheets of dense collagen bundles with sparsely scattered fibroblasts (Fig. 3A, B). And there were some interspersed adipose tissue (Fig. 3C), and entrapped nerve fibers (Fig. 3D). These findings were consistent with those of nuchal-type fibroma. About two years after the operation, there has been no recurrence of the lesion.
DISCUSSION
This case is rare in that it occurred in an uncommon extranuchal site, and interesting in that nuchal-type fibroma was recently described. Clinically, this case resembled lipoma, but physical examination revealed that the lesion had more dense tissue than lipomas. And it had morphologically distinct features from other fibrous tumors.
In 1988, Enzinger and Weiss1 first described nuchal-type fibroma as a rare fibrous growth occurring chiefly in the interscapular and paraspinal regions. Michal et al3 described the clinicopathologic features of 52 cases of nuchal-type fibroma in 1999. The ages of patients ranged from 3 to 68 years, and according to the report nuchal-type fibroma occurs predominantly in males. The nuchal region is the most commonly affected area, but about one-third of cases affected extranuchal sites. Extranuchal sites most often involved the back or scapular region, shoulder, and face. However, other sites of involvement were the forearm, anterior neck, knee, and truncal region.
Macroscopically, nuchal-type fibromas are poorly circumscribed masses with a hard consistency and off-white color. Microscopically, the process was paucicellular and composed of thick, haphazardly arranged collagen fibers. In the central parts of the lesions, the collagen bundles often intersected and had a vaguely lobular architecture. The process was predominantly located in the subcutis, but can exhibit infiltration and entrapment of the underlying fatty tissue or skeletal muscle5. Entrapped islands of adipose tissue were seen in most nuchaltype fibromas, and they contained entrapped peripheral nerve twigs, sometimes exhibiting a splayed appearance similar to that of a traumatic neuroma. A delicate network of elastic fibers was often observed between the collagen fibers3. Extranuchal nuchal-type fibromas were morphologically identical to the examples involving the nuchal region. Our case was consistent with these general findings of nuchal-type fibroma.
Histologic examination of normal tissue from the nuchal region showed thick collagen fibers in the deep dermis reminiscent of those seen in nuchal-type fibroma. However, only the nuchal-type fibromas showed lobulation of the collagen fibers, encasement of adnexal structures, and extensive involvement of the subcutis, resulting in a mass effect. Also, neuroma-like proliferations of the peripheral nerves were not seen in any of the normal tissue specimens3. Nuchal-type fibroma should be distinguished from other fibrous tumors and tumor-like conditions, especially the desmoid-type fibromatosis, circumscribed storiform collagenoma, connective tissue nevus, desmoplastic fibroblastoma, elastofibroma, and fibroma of tendon sheath. Nuchal-type fibroma differ from these tumors in that nuchal-type fibromas are less cellular, poorly circumscribed, and display collagen tissue by bundles of fibers. Treatment of nuchal-type fibroma is surgical excision, but recurrence is common36.
Associated conditions of nuchal-type fibroma have been reported recently. Diabetes is strongly suspected of predisposing the condition of nuchal-type fibroma. In one series, described previously, 44% of patients with nuchal-type fibroma had diabetes3. It suggests that nuchal-type fibroma with diabetes may occur by tumor-like changes in fibrous tissues, like a link between diabetes and scleredema. And, some authors suggested by their case reports that nuchal-type fibroma is related to Gardner's syndrome789. Gardner syndrome, caused by mutations in the adenomatous polyposis coli (APC) gene, is characterized by polyposis coli, osteomas, and various soft-tissue tumors. However, our case did not reveal these associated conditions. The coccygeal area is usually exposed to repeated minor traumas in normal individuals. Thus, this case of the coccygeal location suggests that nuchal-type fibroma can be an abnormal fibrous change against repeated traumas. But, these theories are not yet clearly understood. Therefore, further studies are needed for the etiology of nuchal-type fibromas.

 XML Download
XML Download