

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
The main treatment modality of sinonasal benign tumor is surgical resection, and the endoscopic intranasal approach has been commonly performed since the 1990s. The objective of this study was to evaluate the recurrence rates of different sinonasal benign tumors and to analyze the diverse approaches used in their surgical treatment.
Subjects and Method
In 270 patients who were histopathologically diagnosed with sinonasal benign tumor during a period of 20 years, histopathologic type, treatment approach, interval between first treatment and recurrence, and recurrence rate according to treatment approach were analyzed.
Results
Recurrence rate was higher with the intranasal approach than with the extranasal approach in inverted papilloma and angiofibroma, but the differences were not statistically significant. The proportion of the intranasal approach during the latter 10 years was higher than that during the former 10 years. There was no significant differences between the recurrence rate during the former 10 years and that during the latter 10 years for both intranasal and extranasal approaches.
Figures and Tables


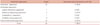
Table 4
Recurrence rate of inverted papilloma according to treatment approach during former 10 years and latter 10 years

*: Patients whose diseases recurred after each period were censored, †: Base period was set on January 1st, 2,000, former 10 years range from January 1st, 1990 until December 31st, 1999 and latter 10 years range from January, 1st 2,000 until December 31st, 2009, ‡: Intranasal approach includes endoscopic approach, microscopic approach, laser vaporization, and modified Denker's operation
![]()


References
1. Ali S, McGarry GW. Endoscopic minimal access surgery in nasal and sinus tumours: lessons from initial experience. Clin Otolaryngol. 2008; 33:42–46.

2. Harvey RJ, Sheahan PO, Schlosser RJ. Surgical management of benign sinonasal masses. Otolaryngol Clin North Am. 2009; 42:353–375.
3. Melroy CT, Senior BA. Benign sinonasal neoplasms: a focus on inverting papilloma. Otolaryngol Clin North Am. 2006; 39:601–617.
4. Tufano RP, Thaler ER, Lanza DC, Goldberg AN, Kennedy DW. Endoscopic management of sinonasal inverted papilloma. Am J Rhinol. 1999; 13:423–426.
5. Lombardi D, Tomenzoli D, Buttà L, Bizzoni A, Farina D, Sberze F, et al. Limitations and complications of endoscopic surgery for treatment for sinonasal inverted papilloma: a reassessment after 212 cases. Head Neck. 2011; 33:1154–1161.
6. Lawson W, Patel ZM. The evolution of management for inverted papilloma: an analysis of 200 cases. Otolaryngol Head Neck Surg. 2009; 140:330–335.
7. Reh DD, Lane AP. The role of endoscopic sinus surgery in the management of sinonasal inverted papilloma. Curr Opin Otolaryngol Head Neck Surg. 2009; 17:6–10.
8. Kim WS, Hyun DW, Kim CH, Yoon JH. Treatment outcomes of sinonasal inverted papillomas according to surgical approaches. Acta Otolaryngol. 2010; 130:493–497.
9. Yoon JH, Kim CH, Choi EC. Treatment outcomes of primary and recurrent inverted papilloma: an analysis of 96 cases. J Laryngol Otol. 2002; 116:699–702.
10. Shin JH, Kim SW, Kim SW, Park CS, Cho JH, Yang MJ, et al. The Usefulness of Endoscopic Management in Benign Sinonasal Tumors. J Rhinol. 2009; 16:39–43.
11. Waitz G, Wigand ME. Results of endoscopic sinus surgery for the treatment of inverted papillomas. Laryngoscope. 1992; 102:917–922.
12. Stankiewicz JA, Girgis SJ. Endoscopic surgical treatment of nasal and paranasal sinus inverted papilloma. Otolaryngol Head Neck Surg. 1993; 109:988–995.
13. McCary WS, Gross CW, Reibel JF, Cantrell RW. Preliminary report: endoscopic versus external surgery in the management of inverting papilloma. Laryngoscope. 1994; 104:415–419.
14. Kamel RH. Transnasal endoscopic medial maxillectomy in inverted papilloma. Laryngoscope. 1995; 105(8 Pt 1):847–853.
15. Busquets JM, Hwang PH. Endoscopic resection of sinonasal inverted papilloma: a meta-analysis. Otolaryngol Head Neck Surg. 2006; 134:476–482.
16. Lawson W, Kaufman MR, Biller HF. Treatment outcomes in the management of inverted papilloma: an analysis of 160 cases. Laryngoscope. 2003; 113:1548–1556.
17. Roh HJ. Inverted papilloma of the sinonasal cavity: the surgical strategy of endoscopic management based on the site of attachment. J Rhinol. 2009; 16:7–11.
18. Eller R, Sillers M. Common fibro-osseous lesions of the paranasal sinuses. Otolaryngol Clin North Am. 2006; 39:585–600.
19. Kim DY, Hong SL, Lee CH, Jin HR, Kang JM, Lee BJ, et al. Inverted papilloma of the nasal cavity and paranasal sinuses: a Korean multicenter study. Laryngoscope. 2012; 122:487–494.
 XML Download
XML Download