

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sleep-disordered breathing (SDB) in children comprises a variety of respiratory disorders including simple snoring, obstructive sleep apnea (OSA), and obstructive hypoventilation (OH). Because SDB is related to many secondary complications with various clinical features, prompt diagnosis and management are necessary in cases of suspected SDB.1)
Among the disorders encompassed within pediatric SDB, OH is characterized by the distinctive clinical feature of an elevated serum concentration of CO2 caused by continuous partial upper airway obstruction during sleep. In OH, there is continuous partial collapse of the upper airway, leading to increased upper airway resistance and hypoventilation, associated with hypercapnia and hypoxemia but without cyclic discrete obstructive events.2) This condition is more common in young children than in adults.2) The definition of OH in children is a syndrome in which the transcutaneous PCO2 or end-tidal PCO2 is greater than 50 mmHg for more than 25% of total sleep time (TST).3)
In terms of SDB in children, many studies have been conducted to date, dealing with the clinical aspects of habitual snoring or OSA. However, there have been few studies regarding the clinical significance and managements in pediatric OH even though it is a unique feature of pediatric SDB. In adult cases, treatment of the cause of the secondary hypoventilation syndrome is recommended, if possible.4) For instance, obesity hypoventilation syndrome (OBS) is known to require proper treatment since it often accompanies with conditions such as heart failure and pulmonary hypertension.5) The treatment of pediatric OH is also necessary for the prevention of chronic CO2 retention and hypoxemia, which are associated with cardiorespiratory morbidity.6) In the present report, we describe two cases of typical pediatric OH that were successfully treated with upper airway surgery.
CASE REPORTS
Case I
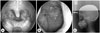
A 12-year-old female patient visited our ear, nose, and throat (ENT) clinic for evaluation of snoring and daytime sleepiness that had begun 1 year earlier. On physical examination, the patient was 145 cm tall and had a body weight of 28 kg with a body mass index (BMI) of 13.3 kg/m2. Upper airway examination revealed no abnormal findings in the nasal cavity and nasopharynx, but bilateral palatine tonsillar hypertrophy was observed (Fig. 1). The patient had no history of other disorders including congenital malformations or central hypoventilation syndrome.
The polysomnography (PSG) conducted at the time of the hospital visit found that the apnea-hypopnea index (AHI) was 0.7/h, the percentage of time out of total sleep time during which blood CO2 was greater than 50 mmHg (PCO2 >50 mmHg/TST) was 34.9%, and the average PCO2 during sleep was 49 mmHg; therefore, the patient was diagnosed with OH. Bilateral tonsillectomy was performed under general anesthesia. The patient experienced no complications such as breathing difficulty or hemorrhage following the surgery.
Twenty-eight months after the surgery, the patient's BMI increased to 18.4 kg/m2, and the OH was improved with an AHI of 0.6/h, PCO2 >50 mmHg/TST of 0.1%, and average PCO2 during sleep of 44 mmHg on PSG (Table 1). Regarding subjective symptoms, snoring was improved from a score of 5 points before surgery (very often) to 0 points (not at all) after surgery on a 7-point Likert scale.
Case II
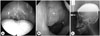
A 16-year-old obese male patient presented to the ENT clinic at the Korea University Ansan Hospital with symptoms of snoring and sleep apnea that had begun 15 years earlier. He was 177 cm tall, weighed 104 kg, and had a BMI of 33.2 kg/m2. Endoscopic examination revealed a nasal septal deviation and oropharyngeal narrowing because of a floppy soft palate, adenoid vegetation, and bilateral tonsillar hypertrophy (Fig. 2).
A PSG was conducted, and the patient was diagnosed with severe OSA with OH. On the PSG, the AHI was 95.1/h, PCO2 >50 mmHg/TST was 27.9%, and average PCO2 during sleep was 42 mmHg. The patient received uvulopalatopharyngoplasty with endoscopic adenoidectomy.
On follow-up evaluation 3 months after the surgery, the patient's BMI was 34.4 kg/m2, which did not represent a significant change from the preoperative BMI of 33.2 kg/m2. However, improvement was observed in the OSA and OH, with an AHI of 7.2/h, PCO2 >50 mmHg/TST of 0.8%, and average PCO2 during sleep of 43 mmHg (Table 1). On a 7-point Likert scale, snoring and sleep apnea were improved from 6 points (all of the time) before surgery to 1 point (rarely) after surgery, and daytime sleepiness was improved from 4 points before surgery (often) to 1 point (rarely) after surgery.
DISCUSSION
Children with SDB often have symptoms such as snoring, apnea, daytime sleepiness, and restless sleep, and the condition may even lead to underdevelopment or behavior problems.7) In children with symptomatic SDB, surgical management such as tonsillectomy and/or adenoidectomy is known to significantly improve respiratory disturbances during sleep.8)
Most SDB studies covering the clinical aspects and surgical treatments are limited to OSA or habitual snoring. In children, OSA due to upper airway obstruction by adenotonsillar hypertrophy is a typical indication for adenotonsillectomy,9) and the efficacy of surgical treatment is well-established.10) However, whether surgical treatment improves clinical symptoms or corrects the PCO2 levels has not been reported in children with OH.11)
The relationship between OSA and OH has been described in a few reports. Normally, patients with OSA can partially compensate for increases in airway resistance, thereby preventing complete upper airway obstruction.12) However, if the compensation is disturbed, it may lead to upper airway collapse, which eventually results in hypoxemia and hypercapnia and gives rise to the OH.2)13) Therefore, as pediatric OSA is improved by the removal of upper airway obstructive lesions, OH can also be considered a condition potentially amenable to surgical management. In this case study, we performed surgical treatment correcting the upper airway obstruction in children with OH diagnosed by PSG. Both patients demonstrated significant improvement in both objective PSG findings and subjective symptoms following surgery.
Although there were clinical symptoms related to upper airway obstruction during sleep, surgical treatment was not indicated in terms of OSA in the first case, since the AHI was in the normal range. Nevertheless, bilateral tonsillectomy was performed for improvement at the obstruction site because the evidence for tonsillar hypertrophy was definitive. Postoperative follow-up results showed that PCO2 was significantly improved along with clinical symptoms. Based on these results, it can be suggested that active surgical treatment may be helpful in patients with pediatric OH syndrome with clinical symptoms and upper airway lesions that may be improved by surgery, even in cases not diagnosed as OSA.
In the first case, the BMI increased from 13.3 kg/m2 to 18.4 kg/m2 after surgery. However according to the 2007 Korean national growth chart, her BMI actually improved from 3rd percentile to 40th percentile curve. This may be due to the correction of sleep disordered breathing after airway surgery which lead to a catch-up growth.
OBS is defined as a state in which blood carbon dioxide concentration upon awakening is greater than 45 mmHg and BMI is greater than 30 kg/m2.14) According to the preoperative PSG (Table 1), the patient in the second case can be regarded as having OBS. In most cases, in the treatment of obesity hypoventilation syndrome, weight loss is considered first. In addition, using a continuous positive airway pressure device and noninvasive mechanical ventilation is recommended.15) However, in the second case of a severely obese child, although the BMI was maintained in the range of severe obesity, it was found that the AHI was improved and the increased PCO2 was normalized over a period of 3 months after adenoidectomy and upper airway surgery of the oropharyngeal soft tissue. These results demonstrate that in the case of upper airway obstructive lesions, OH is improved by surgical treatment even in a patient with obesity hypoventilation.
Thus, in pediatric cases in which there is an upper airway obstructive region amenable to improvement by surgical treatment, proper surgery for the obstructive lesions can be helpful in the amelioration of OH and clinical symptoms. Therefore, upper airway surgery may be considered indicated in cases of OH accompanied by clinical symptoms. Additional research is needed to confirm the effects of surgical treatment and to determine the appropriate surgical indications.

 XML Download
XML Download