

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Primary ciliary dyskinesia is a disease characterized by unexplained neonatal respiratory distress, otitis media, chronic sinusitis, and chronic bronchiectasis. In approximately half of cases, situs inversus totalis or other laterality defects are found. The incidence ranges from 1 in 4,000 to 1 in 40,000 live births. Early diagnosis is important and the disease is finally confirmed by electron microscopic biopsy. The treatment of primary ciliary dyskinesia is based on appropriate procedures. We present a rare case of a 20-year-old male with bronchiectasis, chronic otitis media and chronic sinusitis.
Figures and Tables
Fig. 1
Endoscopic view of the right nasal cavity. A nasal polyp arising from the left middle turbinate (Arrows).
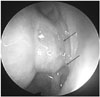
Fig. 2
OMU CT scan (coronal view) reveals soft tissue opacification in both frontal (A), ethmoid, maxillary (B), and sphenoid sinuses (C).

Fig. 3
Chest CT scan (coronal view) shows bronchial wall thickening (arrow) and tram-track sign (arrowhead), suggesting bronchiectasis.

Fig. 4
Temporal bone CT scan (axial view) shows sclerotic changes of the mastoid cavities (arrowheads), normal ossicular chains, and soft tissue filling middle ear cavities (arrows), suggesting bilateral chronic otitis media.



Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Science and Technology and the Ministry of Science, ICT & Future Planning (NRF-2016R1E1A2020731, 2017R1A2B2003575) and a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C0387). This research was also supported by a grant of Korea University Medical Center and Anam Hospital, Seoul, Republic of Korea (O1700021).
References
1. Horani A, Ferkol TW. Primary ciliary dyskinesia and associated sensory ciliopathies. Expert Rev Respir Med. 2016; 10(5):569–576.

2. Lewis WR, Malarkey EB, Tritschler D, Bower R, Pasek RC, Porath JD, et al. Mutation of Growth Arrest Specific 8 Reveals a Role in Motile Cilia Function and Human Disease. PLoS Genet. 2016; 12(7):e1006220.
3. Mitchison HM, Valente EM. Motile and non-motile cilia in human pathology: from function to phenotypes. J Pathol. 2017; 241(2):294–309.
4. Lucas JS, Burgess A, Mitchison HM, Moya E, Williamson M, Hogg C. Diagnosis and management of primary ciliary diskynesia. Arch Dis Child. 2014; 99:850–856.
5. Park CW, Koh JS, Kim KR, Lee HS. A Clinical Study on Primary Ciliary Dyskinesia. Korean J Otolaryngol-Head Neck Surg. 1997; 40:1079–1084.
6. Shin SA, Yang S, Oh JW, Lee HB, Park CE, Kwan JK. Ultrastructure of nasal cilia in children with recurrent or persistent respiratory diseases. Korean J Pediatr. 2006; 49:410–416.
7. Hogg C. Primary ciliary dyskinesia: when to suspect the diagnosis and how to confirm it. Paediatr Respir Rev. 2009; 10:44–50.
8. Popatia R, Haver K, Casey A. Primary Ciliary Dyskinesia: An Update on New Diagnostic Modalities and Review of the Literature. Pediatr Allergy Immunol Pulmonol. 2014; 27(2):51–59.
9. Storm van's Gravesande K, Omran H. Primary Ciliary Dyskinesia: clinical presentation, diagnosis and genetics. Ann Med. 2005; 37(6):439–449.
10. Ryu JS, Jeong DW, Park YK, Kim KS. A Case of Kartagener's Syndrome Combined with Congenital Nystagmus. Korean J Otolaryngol-Head Neck Surg. 2001; 44:657–661.
11. Leigh MW, O'Callaghan C, Knowles MR. The challenges of diagnosing primary ciliary dyskinesia. Proc Am Thorac Soc. 2011; 8(5):434–437.
12. Walker WT, Jackson CL, Lackie PM, Hogg C, Lucas JS. Nitric oxide in primary ciliary dyskinesia. Eur Respir J. 2012; 40(4):1024–1032.
13. Corbelli R, Bringolf-Isler B, Amacher A, Sasse B, Spycher M, Hammer J. Nasal nitric oxide measurements to screen children for primary ciliary dyskinesia. Chest. 2004; 126(4):1054–1059.
14. Jackson CL, Behan L, Collins SA, Goggin PM, Adam EC, Coles JL, et al. Accuracy of diagnostic testing in primary ciliary dyskinesia. Eur Respir J. 2016; 47(3):837–848.
15. Knowles MR, Daniels LA, Davis SD, Zariwala MA, Leigh MW. Primary Ciliary Dyskinesia. Recent Advances in Diagnostics, Genetics, and Characterization of Clinical Disease. Am J Respir Crit Care Med. 2013; 188(8):913–922.
16. Bush A, Cole P, Hariri M, Mackay I, Phillips G, O'Callaghan C, et al. Primary ciliary dyskinesia: diagnosis and standards of care. Eur Respir J. 1998; 12:982–988.
17. el-Sayed Y, al-Sarhani A, al-Essa AR. Otological manifestations of primary ciliary dyskinesia. Clin Otolaryngol Allied Sci. 1997; 22(3):266–270.
 XML Download
XML Download