

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multi-drug resistant tuberculosis (MDR-TB) is a major health problem that threatens the success of tuberculosis (TB) control programs worldwide [12]. The World Health Organization (WHO) launched the global surveillance project for anti-TB drug resistance in 1994 [1]. An estimated 3.3% (2.2-4.4%) of new cases and 20% (14-27%) of repeat TB cases were caused by MDR-TB in 2014, consistent with recent years [1]. In 2014, an estimated 480,000 people worldwide developed MDR-TB, and 190,000 people died as a result [1]. MDR-TB is caused by strains of Mycobacterium tuberculosis that are resistant to both isoniazid (INH) and rifampicin (RFP), the two most potent TB drugs.
In 1965, the incidence of TB in South Korea was 668 cases per 100,000 [3]. Since the implementation of standardized therapeutic approaches in the 1980s, the prevalence of TB and MDR-TB has decreased [4, 5]. According to a national survey of drug-resistant TB in South Korea, the prevalence of MDR-TB has decreased from 23.8% in 1980 to 5.8% in 1995 in people with new cases, and from 27.5% in 1994 to 7.1% in 1998 in people who had previously been treated for TB [45].Although this decline continued in 2015, with the prevalence of new MDR-TB cases at 2.4% [6], South Korea continues to have one of the highest burdens of MDR-TB in member countries of the organization for economic co-operation and development (OECD) [16].
According to WHO, the MDR-TB treatment success target of > 75% was reached by 43 of the 127 countries in 2012 [1]. The treatment of MDR-TB patient is usually complex and less effective than treating drug-sensitive TB, and the optimal composition and duration of MDR-TB treatment regimens is uncertain [12]. Despite the global effort to control MDR-TB, the success rates of treatment continue to show insufficient results. There is also a lack of information about risk factors for adverse outcomes in patients with MDR-TB in South Korea.
We performed a retrospective cohort study to reveal the clinical outcomes and risk factors associated with poor outcome in MDR-TB patients.
METHODS
Patients
We retrospectively and consecutively evaluated all patients who were registered at a single TB-specialized hospital in South Korea from January 2005 to February 2011. All patients were initially treated as inpatients, but some of them were followed-up with as outpatients after hospitalization. All patients had sputum specimens positive for M. tuberculosis, along with smears, cultures, and drug susceptibility tests (DST) at the time of diagnosis. Patients were diagnosed with MDR-TB if the DST results showed resistance to at least both INH and RFP. We reviewed patients' medical records for demographic information, previous TB treatment, comorbidities, DST results, chest radiographs, treatment regimens, and clinical outcomes. The clinical outcomes of MDR-TB followed the international consensus guidelines [78]. This study was approved by The Ethics Committee of the National Masan Tuberculosis Hospital of the National Institutes of Health.
Laboratory methods
Sputum specimens were processed using NaOH and N-acetyl-L-cysteine for screening of acid-fast bacilli using the Ziehl-Neelsen method. All cultures were performed using the MB/BacT liquid culture system (bioMerieux Inc., Durham, NC, USA) and Ogawa agar slants (egg-based medium; Shinyang Chemical, Korea). The DSTs were performed using Lowenstein-Jensen agar slants at the following antibiotic concentrations: rifampicin (40 mg/mL), isoniazid (0.2 mg/mL), ethambutol (2.0 mg/mL), kanamycin (40 mg/mL), streptomycin (10 mg/mL), ofloxacin (2.0 mg/mL), ethionamide (40 mg/mL), para-aminosalicylic acid (PAS; 1mg/mL), and cycloserine (30 mg/mL). The resistance of other drugs was defined as > 1% growth in Lowenstein-Jensen media.
Treatment
The national guidelines for treating TB are based on DST results and patients' history of drugs taken. Treatments were started and modified following discussions among a team of specialists. The typical regimen consisted of at least four susceptible oral drugs and one injectable drug. If possible, the four oral drugs were used for the full treatment period, and the injectable drug was used for 8 months at a frequency of six times per week for the first 2 months, and then three times per week for the remainder of the treatment period. Renal function, hepatic function, sputum smears, and cultures were assessed by monthly until the end of treatment. The typical duration of treatment was 12-36 months, depending on culture results, changes in chest radiographs, and history of TB treatment.
Data collection
All patient information was collected and recorded by attending physicians. We extracted demographic and risk factor information, age, sex, alcohol use, body mass index (BMI), comorbidities, chest radiographs, history of TB, surgical history for TB, the number of susceptible drugs, the number of drugs used for ≥2 months, treatment duration, side-effects, and response to treatment.
Definitions
We defined MDR-TB according to the standard classifications [12]. The clinical outcomes of MDR-TB followed the international consensus guidelines [7]. A “cured” patient was defined as having completed their treatment as recommended by the national policy without evidence of failure, and three or more consecutive TB-negative cultures, taken at least 30 days apart. A patient classified as “completed” was defined as having completed treatment as recommended by the national policy without evidence of failure, but with no record of three or more consecutive TB-negative cultures. The “defaulted” category was comprised of patients whose treatment was interrupted for two or more consecutive months. Patients classified as “treatment failed” had their treatment terminated or needed a regimen change affecting at least two anti-TB drugs due to: 1) lack of culture conversion (from TB-positive to TB-negative) by the end of the intensive phase, 2) bacteriological reversion in the continuation phase after conversion to TB-negative, 3) evidence of additional acquired resistance to fluoroquinolones or second-line injectable drugs, or 4) adverse drug reactions. Patient mortality was classified under the category “died”. Successful outcomes were defined as the combination of “cured” and “completed treatment”, while “defaulted”, “treatment failed”, and “died” were used as a composite variable for poor outcome.
Statistical analysis
All statistical analyses were conducted using SPSS software, version 14.0 (SPSS, IL,Chicago). Missing data were not replaced or imputed. We calculated p values using Fisher's exact or Pearson's Chi-square tests, and significance was set to < 0.05. To evaluate the risk factors for poor outcome, we used Cox proportional-hazard regression analysis. In the multivariate model of efficacy (from which defaulters were excluded) we included relevant variables with p values < 0.50 in the univariate analysis. We calculated associations between the variables included in multivariate analysis, again setting p values < 0.05 as statistically significant.
RESULTS
Patient demographics
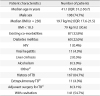
We included 258 patients in our study who were registered with a TB-specialized hospital in South Korea from January 2005 to February 2011. All demographic data is presented in Table 1. The patients' median age was 41.1 years (interquartile range [IQR]: 31.2-50.7); 193 patients (74.8%) were men, with a median age of 41.1 years (IQR: 32.6-50.3). MDR-TB was found in 167 patients (64.7%) treated for TB. Median BMI in all patients was 19.7 kg/m2(IQR: 17.6-21.5), and 30.6% of patients were defined as underweight (BMI < 18.5 kg/m2). Comorbidities were present in 87 patients (32.8%): 60 patients (22.6%) had diabetes mellitus, 11 (4.3%) had viral hepatitis, two (0.5%) had liver cirrhosis, and one was infected with human immunodeficiency virus (HIV). Further, 11 patients had extrapulmonary involvement such as TB meningitis, TB enteritis, and TB spondylitis. Lung cavitation was confirmed with chest radiography in 141 patients (54.7%), and eight (3.1%) received adjuvant surgical treatment: two patients underwent a wedge resection procedure, and six patients had lobectomies.
Clinical characteristics
The median treatment duration was 24 months (IQR: 18-24). Ninety patients (34.9%) experienced side-effects due to treatment, with the most common being gastrointestinal problems, such as nausea, vomiting, and abdominal pain. One patient discontinued treatment because of adverse side-effects; this patient was classified as “treatment failure”. At the initial treatment, 220 patients (85.3%) were confirmed TB-positive on sputum cultures. At the start of treatment, the degree of drug susceptibility varied; the mean number of drugs to which M. tuberculosis was susceptible at treatment onset was 4.5 ± 1.0 (Table 2).
Drug resistance and treatment
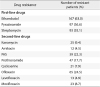
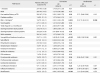
The 258 patients received different empirical initial treatments. In the first 2 or more months, the most commonly used drugs were prothionamide, cycloserine, PAS, levofloxacin, pyrazinamide, ethambutol, moxifloxacin, and ofloxacin; kanamycin or streptomycin were commonly used as the injectable drugs (Table 3). Ethambutol was the most common drug to which patients were resistant, experienced by 63% of patients. Resistance to second-line anti-TB drugs like ofloxacin, PAS, and prothionamide was common in all patients (Table 4).
Treatment outcomes
The overall success rate of MDR-TB treatment was approximately 86% (222 patients), with 14% (37 patients) of patients experiencing poor treatment outcomes. Of the total participants, 207 (80.2%) were cured, 15 (5.8%) completed treatment, 29 (11.3%) were classified as having failed treatment, six (2.3%) died, and one (0.4%) defaulted (Table 5).
Predictors of poor treatment outcomes
Univariate Cox proportional-hazards analysis showed that poor outcome was significantly associated with low BMI (Hazard ratio [HR]: 2.92; 95% Confidence interval [CI]: 1.5-5.7, p = 0.002), history of TB treatment (HR: 2.49; 95% CI: 1.09-5.72, p = 0.031), susceptibility to four or fewer drugs at treatment onset (HR: 5.49; 95% CI: 2.42-12.54, p < 0.001). Resistance to a pyrazinamide (HR: 1.97; 95% CI: 1.02-3.79, p = 0.043), levofloxacin (HR: 3.34; 95% CI: 1.17-9.56, p = 0.024), moxifloxacin (HR: 4.1; 95% CI: 1.95-8.56, p < 0.001), and ofloxacin (HR: 5.35; 95% CI: 2.72-10.52, p < 0.001) were also significantly associated with a poor outcome. In the multivariate Cox proportional-hazards regression analysis, three factors remained significantly related to poor outcome: susceptibility to four or fewer drugs (HR: 3.89; 95% CI: 1.38-10.96, p = 0.01), resistance to ofloxacin (HR: 2.49; 95% CI: 1.06-5.81, p = 0.035), and a BMI < 18.5 kg/m2 (HR: 2.57; 95% CI: 1.28-5.15, p = 0.008).
DISCUSSION
We analyzed patients' demographics, clinical features, resistance to anti-TB drugs, and treatment regimens to investigate factors associated with poor outcome for patients with MDR-TB. Approximately 35.3% of our patients did not receive any prior TB treatment. The proportion of MDR-TB patients in our South Korean cohort with resistance to ofloxacin was 24.5%, higher than 4% reported in Latvia [8]. We combined patients who were cured and who had completed their treatment into one category — successful outcomes — and all other patients were categorized as poor outcome. The overall rate of successful outcome was approximately 86.0%, which exceeds that of many other countries [1]. The risk factors for poor outcome in MDR-TB infection and treatment were identified as low BMI, ofloxacin resistance, and being susceptible to four or fewer drugs at treatment initiation.
Other studies have also found that individuals who are underweight (BMI < 18.5 kg/m2) at the start of MDR-TB treatment have a high risk for poor outcome [8910]. Leimane et al have reported that BMI < 18.5 kg/m2 at the start of MDR-TB treatment is associated with death and treatment failure in Latvia (HR: 2.3, 95% CI: 1.1-4.9, p = 0.03) [8]. Putri et al. have suggested that MDR-TB patients who are severely underweight (BMI < 16 kg/m2) experience longer time to initial sputum culture conversion from TB-positive to TB-negative (HR: 0.55, 95% CI: 0.37-0.84, p = 0.002) [10]. Our findings are consistent with these, since we found that poor MDR-TB treatment outcomes were associated with a BMI < 18.5 kg/m2 (HR: 2.569; 95% CI: 1.281-5.152, p = 0.008), suggesting that malnutrition may impair host immunity against M. tuberculosis, and that nutritional status might be an important predictor of treatment outcome.
Mauara et al. have shown that DST results for anti-TB drugs are associated with treatment outcomes [11].Among 8,955 analyzed patients, DST results were significantly associated with higher odds of successful treatment if sensitive drugs are used in the treatment regimen [11]. Ahuja et al. suggested that it would be appropriate to use at least four drugs that are recognized as likely to be effective from DSTs during the initial intensive phase, when standardized regimens are used with routine DSTs [12]. The data from our analysis showed that the number of MDR-TB drugs to which patients are susceptible, particularly when they are susceptible to four or fewer drugs, could be risk factor for poor outcome. This finding suggests that DST results can be useful for selecting anti-TB drugs in personalized MDR-TB treatments.
The fluoroquinolones were found to have good in vitro activity against M. tuberculosis in the 1980s, and subsequent studies have showed in vivo efficacy thereafter [1314]. Fluoroquinolones have therefore been recommended as second-line antibiotics for MDR-TB management. Previous studies have also showed that resistance specifically to the fluoroquinolone ofloxacin is also predictive of poor outcome [815]. Our results found a significant association between ofloxacin resistance and poor outcome (HR: 2.485; 95% CI: 1.064-5.805; p = 0.035). Yew et al. showed that in vitro resistance to ofloxacin is independently associated with adverse outcomes (p < 0.05; Odds Ratios = 15.9, 13.5, 12.8) [15]. The authors suggested that most MDR-TB patients can be treated effectively with regimens of both ofloxacin and levofloxacin. In the present study, the proportion of patients with resistance to ofloxacin was 24.5%, much higher than the 4% reported in Latvia [8]. This higher proportion may be due to the widespread use of fluoroquinolones for treating bacterial respiratory disease in South Korea.
Our study has several limitations. All the patients were selected from a single referral center in South Korea, which may have introduced selection bias. Thus, the findings cannot be assumed to be fully representative of the clinical characteristics and current situation of MDR-TB in South Korea; rather, these findings may represent TB in specialized TB hospitals. This study also had a small sample size for cases of treatment failure. A larger sample size could better corroborate the treatment outcomes and the predictors for poor MDR-TB outcomes. Another limitation is that we were unable to demonstrate why low BMI is associated with poor outcome. Being underweight may be marker for poverty, and poor patients may experience more difficulties in accessing routine treatment. TB may also be one of the most frequent causes of wasting [1317].Furthermore, previous studies and the WHO have recommended the use of moxifloxacin in ofloxacin-resistant patients [18], but we did not analyze the use of alternate fluoroquinolone regimens in patients resistant to ofloxacin. Finally, prior TB treatment is a well-known risk factor for poor outcomes for patients with MDR-TB, potentially because the duration of treatment may be responsible for resistance to second-line drugs [81920]. We did not find prior TB treatment to be a major factor for poor outcome; this could be because we did not assess the drug history of all patients into TB and MDR-TB.
Despite those limitations, this study represents an important investigation of the characteristics and risk factors associated with poor outcome for patients with MDR-TB in South Korea. Our study showed that being underweight (BMI < 18.5 kg/m2), being susceptible to four or fewer drugs at the start of treatment, and ofloxacin resistance were independent risk factors for poor outcome in MDR-TB patients. Comparisons of these findings with other reports will contribute to the enhancement of treatment and management approaches for patients with MDR-TB.



 XML Download
XML Download