

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tinnitus is the hearing of sound mostly within one's ears or sometimes within one's head, without external acoustic stimulus. Tinnitus is a common symptom, which can often be easily cured through medication, noise masking, or psychotherapy, but 10% of cases are considered intractable, causing patients to suffer from insomnia, interference with concentration, and hearing disturbance. If left uncured, tinnitus may cause hearing loss, so efforts should be made for its treatment using methods such as medication, sound generators, hearing aids, local anesthesia, local steroid injection, and psychological therapy. Still, some cases are diagnosed as intractable tinnitus, in which case doctors often give up its treatment.
Some cases of intractable tinnitus are caused by compression on auditory nerves by the artery at the brainstem root entry zone of the nerve, in which case microvascular decompression (MVD) is often used as a treatment [123]. However, the effects of MVD on intractable tinnitus have been reported to be less extensive than on hemifacial spasm or trigeminal neuralgia. No clear criteria have yet been established for surgical treatment of intractable tinnitus [3]. Moreover, the operation involves direct maneuver of the auditory nerves, increasing the chance of postsurgical hypofunction of the nerves. Thus, more advanced microsurgical instrumentation and consistent intraoperative monitoring of the brainstem auditory evoked potential (BAEP) have been introduced to significantly reduce the chance of hearing loss [45].
THEORETICAL FOUNDATIONS AND RESULTS OF MVD
Janetta suggested that whether the vessels are large or small, normal or abnormal, they could all cause trigeminal neuralgia, pointing to neurovascular compression as the main cause of tinnitus, and conducted MVD on tinnitus cases [2]. There are two common causes of cranial nerve disorders such as trigeminal neuralgia, hemifacial spasm, and geniculate otalgia [6]. One is hyperexcitability, and the other is ephaptic transmission. Cranial nerves often get hyperexcited if they are damaged by brain vessels, bones, or a tumor, while it is well known that the major cause of the development of trigeminal neuralgia is hyperexcitement of the nerves. If a nerve axon is damaged over a long period of time, it develops sensitivity to compression, and relaxed discharge could cause trigeminal neuralgia, causing nerves to become hyperexcited with even subtle stimulation. According to Calvin et al. [7], pain from trigeminal neuralgia is caused by electrical synaptic transmission that takes place around the area where vessels contact the nerves, which causes abnormal nerve movement by the interdigitation from the movement of the subtly damaged neurofiber. On the other hand, others claim that trigeminal neuralgia occurs for complex reasons including peripheral abnormality (i.e. nerve compression) and central abnormality (i.e. hypokolasia of trigeminal nucleus), presenting cases where vascular compression did not lead to trigeminal neuralgia [89]. Similarly, it makes more sense to see vascular compression as one of many causes that lead to hemifacial spasm, rather than seeing it as the only cause. The central origin plays a part in the development and maintenance of the condition. This explains why it is not possible for symptoms to occur without the role of the central origin, even under vascular compression [810].
Tinnitus is also caused by ephaptic transmission or hyperexcitement, as well as central abnormality of the acoustic nerve nucleus, which compresses other abnormal signals. Moller proposed the existence of a secondary cause, based on experience treating tinnitus with medication [11]. Moller noted that a secondary cause plays a role in the development of the symptoms, even under vascular compression, and vascular compression itself would not cause the symptoms without a secondary cause. He proposed that fatigue, vitamin deficiency, brain atrophy by aging, and direct physical injury were potential secondary causes, on the grounds that tinnitus is rare among young patients. He recommended surgical procedure for types of tinnitus that cannot be cured through medication.
The prognosis of MVD operations on tinnitus cases may depend on the duration of the follow-up period and the definition of a successful surgical outcome. According to Yap et al. [12], success rates for surgery reported by different studies vary from 27.8% to 100%. Moller et al. [3] suggested a number of empirical reasons why some MVD operations have been unsuccessful. First, not all patients who underwent the surgery may not have had compression of the auditory nerve. The causes of tinnitus can be diverse and complex, so precise radiological examination and special caution by surgeons are required in deciding on candidates for MVD. Second, the offending artery may not have been properly decompressed during surgery. MVD surgeries require an advanced level of surgical maneuvering; substantial experience and extra attention are necessary for proper decompression. Third, the acoustic nerve may have undergone postoperative damage through excessive decompression, which can be effectively prevented by constant intraoperative monitoring of the BAEP. Fourth, a remarkably long recovery time is needed for the compressed nerve, so early follow-up may result in low apparent success rates. Fifth, numerous studies have shown that the duration of the condition affects the surgical outcome [151619]. The longer the duration before intervention, the less effective the results of the surgery have been, similar to what can be seen in cases of trigeminal neuralgia. Surgery should be carried out within 6 years of the development of the symptoms for better results.
Moller et al. [3] reported on a study of 72 patients treated over a period of 10 years, with an average follow-up period of 1.9 years, that 29 of them (40.3%) were completely cured or saw remarkable improvement. In the study by Ko and Park [5], the rate was 78.6%, a better performance than Moller et al. [3] saw, thanks to more advan c ed MVD technology, more careful selection of the subjects, operation by a single surgeon, and constant intraoperative BAEP level monitoring: Specifically, extra caution was taken when wave V of the auditory brainstem potential was 0.5 ms or longer, and the surgery was suspended if it reached 1 ms or longer or a sudden shrink of the amplitude occurred. Recently, Zhang et al. [14] reported on a study conducted on 37 patients, in which 22 of them saw disappearance of tinnitus right after surgery, 14 after an average of 18.6 months (ranging from 12 to 29 months), 7 partial disappearance after the same period, and 4 no effect, demonstrating a total cure rate of 56% and effective rate of 84%. They suggested the following five rules for a successful MVD operation on tinnitus: 1) The flocculus of the cerebellum and the acoustic nerve must be detached carefully in order to reduce the excessive traction effect inflicted on the acoustic nerve. 2) The anterior inferior cerebellar artery and the internal auditory artery should not be pulled. 3) The BAEP levels must be monitored during the procedure, and the operation should be halted if the P5 amplitude falls, until it recovers to within normal range. 4) If the latency lasts 1 ms or more, compound action potentials (CAPs) should be measured. 5) Endoscopy may be used to find the offending vessel and protect perforating arteries.
An attempt was made to record the level of noise felt by tinnitus patients in order to choose appropriate candidates for MVD surgery. According to Brookes, a relative tinnitus level ("Tr") can be measured by subtracting the pure tone level (At) from the relative noise level (Ts). If "Tr" is 25 dB or louder, psychological problems may occur, while substantial noise can be perceived between 25 dB and 35 dB, and extreme noise at 40 dB and louder [15]. The average Tr value of the 9 subjects was 43 dB (highest: 60 dB, lowest: 35 dB), meaning most of the tinnitus patients had a Tr level which can cause psychological issues, perceiving extreme noise that affects daily activities. In the study by Ko and Park [5], the average Ts was 82 dB, that of At 40 dB, and that of Tr 42 dB, indicating that all subjects were suffering from extreme noise and requested surgery.
THE OFFENDING ARTERY
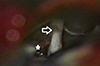
Ko and Park [5] reported that in most cases, the anterior inferior cerebellar artery (AICA) was the root cause of the tinnitus development—being the only cause in a majority, and in the remaining of these cases working in combination with a vein. The posterior inferior cerebellar artery and the labyrinthine artery were the root cause in less than 10% of the cases, while vein was the only cause in a small number of cases. Vasma et al. [16] pointed to the AICA or both AICA and vein as the offending vessels causing compression in 17 of the 22 cases. In cases where a vein was the cause, it was swollen to more than five times the normal size, causing damage to the acoustic nerve because the pulsatile vessel wraps around the entrance zone of the nerve. In some cases, local thinning or discoloration of the compressed nerve was observed, in which cases the tinnitus improved right after surgery, indicating that the root cause was vascular compression (Fig. 1).
INTRAOPERATIVE MONITORING OF EVOKED POTENTIALS
The evoked potential is an electrical potential recorded from the nervous system following presentation of a motor or sensory stimulus after a certain latency. The concept was introduced into clinical practice during the early 1970s, used as a non-invasive method during the processes of diagnosis and treatment of many diseases. Clinically, somatosensory, brainstem auditory, and visual evoked potential are the most common. Brainstem auditory evoked potentials (BAEPs) are far-field reflections recorded in response to repetitive clicking sounds from electrodes placed on the scalp, representing neuronal activity. In 1967, Sohmer and Feinmesser first measured the BAEPs of humans [17], and since then the method has been used clinically in neurology and audiology for diagnosis and audiometry, and more recently in the neurosurgery field for diagnosis and intraoperative monitoring of posterior fossa lesions.
Levin et al. [18] first recorded the BAEP intraoperatively in 1978, proving that a constant recording during surgery is possible, as it is rarely affected by anesthesia, while providing information on functional changes of the nervous system, helping improve prediction of the risk of damage to the acoustic nerve or brainstem structure. However, it should be taken into account that a combination of factors including the level of anesthesia, body position, body temperature, blood pressure, patient's age, gender, the strength of auditory stimulus play a role in intraoperative BAEP for more precise analysis.
During posterior fossa lesion surgery, complications such as hearing disorder or brain stem damage may occur, especially when maneuvering the cerebellopontine angle area, due to cerebellum traction or ischemic injury caused by direct maneuvering of the acoustic nerve [11]. Approximately 1-4% of patients with trigeminal neuralgia or hemifacial spasm experience complete postoperative hearing loss, while 20% may suffer partial hearing damage. Studies have been carried out on the effectiveness of measuring BAEPs as an intraoperative monitoring method to prevent these complications from taking place. In 1982, Grundy et al. [20] discovered meaningful fluctuations of waves in 31 of the 37 cases of cerebellopontine angle operations, 22 during double cerebellum traction, 3 during maneuvering of the brain stem or the acoustic nerve, and 6 when the body position was fixed. As such, a majority of damage is caused by cerebellum traction and maneuvering of the brain stem or acoustic nerve, indicating the necessity of monitoring BA EPs. Ojemann et al. [21] reported that they were able to protect the acoustic nerve in 21 out of 22 cases by measuring intraoperative BAEPs to preserve hearing acuity during acoustic neuroma removal surgery. Zappulla et al. [22] also supported the effectiveness of BAEPs in the same procedure, reporting that they could easily determine whether the acoustic nerve was being damaged during the process of cerebellum traction, internal acoustic canal compression, and detachment of the acoustic neuroma by constantly observing BA EPs, resulting in avoiding any postoperative hearing loss. Moller et al. [4] highlighted the effectiveness of intraoperative BAEP measurement in their research, reporting just 4 cases of hearing loss out of 140 MVD cases.
In 1982, Raudzens and Shetter found 46 cases in which the intraoperative latency of waves III and V were 1.0 ms or longer during posterior fossa lesion operation as abnormal, and changed the operational method to avoid further damage of the acoustic nerve. As a result, 7 cases with just delay of latency demonstrated no hearing loss, while 4 patients in which all auditory brainstem potential waves disappeared after wave I experienced permanent hearing loss. They concluded that only cases where all waves disappeared led to postoperative hearing disorder, while delay of latency itself is likely to be a false positive, with no need of changing the type of operation [23]. Grundy et al. [20] measured intraoperative BAEP in 54 cerebellopontine angle surgery cases including 42 MVD cases, classifying a wave V latency delay of 1.5 ms or longer as abnormal. They found clinically meaningful changes in the waves in a total of 37 cases, 32 of them reversible and 5 of them irreversible, with only the latter leading to postoperative hearing loss. Little et al. [24] maintained that intraoperative wave V latency of 0.5 ms or more should be considered abnormal and be reported to the surgeon, while Schramm et al. [25] suggested that a decrease of more than 50% of the maximum amplitude is more meaningful than a reversible increase in latency with regard to postoperative hearing loss, after studying 31 posterior fossa lesion surgical procedures. Hatayama et al. [26] evaluated 38 out of 350 MVD cases for which intraoperative wave V latency was 1.0 ms or longer to discover its correlation with hearing ability. They found that 12 of the patients experienced hearing loss, and in particular, 11 of those whose wave V amplitude decreased by 40% or more showed hearing loss, meaning it was a more reliable criterion than simple delay of latency.
PREOPERATIVE DETERMINANTS
Ko and Park [5] found that tinnitus cure rates were higher among the patient group with normal preoperative BAEP levels (P=0.000) than those with abnormal preoperative BAEP levels. Moreover, at 1.5-year short-term follow-up, they found the following preoperative determinants of a successful surgical outcome: patient age of 45 and under (P=0.021); 6 years or less duration of tinnitus (P= 0.017); normal BAEP (P=0.002); loop type of offending anterior inferior cerebellar artery (P=0.043); and nonexistence of vertigo (P=0.018).
There are various factors that lead to the development of tinnitus, and many times multiple factors work in combination, so precise radiological examinations and caution from surgeons are required before selecting candidates for MVD surgery. High-performance MRI machines should be used to scan the precise structure of the artery, using the TOF technique and 1-mm overlap to observe the acoustic nerve and nearby artery. Teflon sheets should be inserted between the vessel and the nerve during MVD surgery, but an excessive number may lead to damage of the nerve, causing hearing deterioration or loss, while too few may show no decompression effect. The amount of Teflon should be adjusted intraoperatively in accordance with the BAEP level, and should be reduced in case of a sudden fluctuation of the level. The nerve could be da maged postoperatively even after a successful MVD surgery, while constant monitoring of intraoperative BAEP could effectively prevent damage of the nerve caused by excessive decompression. The prognosis of the surgery is also highly related to the duration of the tinnitus. Ko and Park [5] proposed performing the surgery within 6 years of the advent of symptoms, noting that the longer the patient had been suffering from tinnitus, the less effective the surgery was—a similar phenomenon to that which occurs with surgery performed for trigeminal neuralgia. Meanwhile, the success rate was higher among younger patients, as aging of the nervous system may work as a secondary cause leading to tinnitus development. Patients whose surgery was ineffective could hope for improved results with time, as can be seen in trigeminal neuralgia cases. Meanwhile, patients should not be exposed to noise, fatigue, or heavy drinking after surgery since the acoustic nerve is relatively weak at that time.
CONCLUSION
Currently, in most cases of intractable tinnitus that cannot be cured with palliative treatment, doctors often give up on physical treatment and instead take a psychological approach. However, if a precise examination points to acoustic vascular compression as the main cause, the symptoms are highly likely to be cured with MVD surgery, with an especially good prognosis if the candidates for this procedure are selected with extra caution. Preoperative determinants are age, normal/abnormal preoperative BAEP, the duration of symptoms, and the relationship between the acoustic nerve and the artery. Incessant monitoring of intraoperative BAEPs could prevent postoperative hearing loss.
 XML Download
XML Download