

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Over the years, smaller and more immature infants are more likely to be surviving. The improvement of survival rates in very preterm infants is closely correlated with the development of new technology in prenatal care medicine, especially in ventilation therapy. Recent advances in neonatal ventilation therapy have changed the epidemiology of bronchopulmonary dysplasia (BPD), a major morbidity among preterm infants, since it was originally described by Northway.1 While recent BPD shows a milder form of clinical presentation, the incidence of BPD has been increased during past decades.1
The pathogenesis of BPD is multi-factorial2 and the causes include mechanical ventilation-induced lung injury (VILI).3, 4 Various connotations have been used to describe components of VILI, which may be interrelated and may act synergistically. Volutrauma refers to the damage caused by overdistension of the lung by the delivery of too much gas. Barotrauma, or excessive pressure, may damage airway epithelium and disrupt alveoli. Atelectotrauma refers to the damage caused by the continual opening and closing (the cycle of recruitment and subsequent de-recruitment) of lung units. Biotrauma is a collective term to describe the injurious effects of infection, inflammation and/or oxidative stress on the developing lung. So the development of lung protective strategies for preterm infants is a major issue in neonatal intensive care medicine.5
Here I introduce new modalities and modes in neonatal ventilation therapy, which were developed with the purpose of reducing VILI and improving long-term clinical outcomes.
New Modalities in Non Invasive Ventilation
Non invasive ventilation (NIV) is increasingly being used in preterm infants to reduce the risk of adverse effects associated with invasive mechanical ventilation via endotracheal tube.6, 7 Because it is well known that the duration of mechanical ventilation via endotracheal tube has a direct correlation with BPD, non invasive ventilation methods including nasal continuous positive airway pressure (nCPAP) and nasal intermittent positive pressure ventilation (NIPPV) have been tried to reduce the duration of invasive ventilation.8, 9 nCPAP can be delivered using conventional mechanical ventilators, bubble CPAP or infant flow drive system. High-flow (>2 L/min) nasal cannulae are used to deliver CPAP in some centers. The infant flow driver uses a fluidic flip system which has been shown to assist spontaneous breathing and reduce work of breathing by reducing expiratory resistance and maintaining a stable airway pressure throughout the respiratory cycle. nCPAP appears to be beneficial in the management of apnea of prematurity and for prevention of extubation failure.10 However from the point of view as the early ventilatory management, nCPAP has limitations. nCPAP has been used for this purpose early in the respiratory course, but a significant proportion of the smaller infants fail. As reported in the COIN trial 55% of infants born at 25~26 weeks gestation and 40% of 27~28 weeks failed N-CPAP during the first 5 days and required intubation.11 A major cause of failure of nCPAP is the need for intubation due to uncontrollable apnea, bradycardia or desaturation in preterm infants.11 NIPPV is an alternative option when infants are extubated from IVET or for infants failing nCPAP. NIPPV is a form of NIV that combines nCPAP with IPPV breaths.12 NIPPV may be more promising than nCPAP in prevention of postextubation failure, minimizing SIMV duration and potentially decreasing the incidence of BPD.13, 14 NIPPV has been shown to decrease postextubation failure significantly compared to nCPAP. Two randomized studies using synchronized NIPPV at the time of extubation showed significant reduction in extubation failure with NIPPV compared to NCPAP.15, 16 Furthermore a retrospective study showed that the introduction of NIPPV could reduce BPD rates significantly. Also recent studies comparing NIPPV and SIMV have shown promising results. Kugelman et al. compared nCPAP with NIPPV as a primary mode of respiratory support in preterm infants less than 35 weeks' gestational age with RDS and NIPPV was more successful than nCPAP in decreasing the need for endotracheal intubation and the incidence of BPD was lower.16 No adverse effects of NIPPV were reported in these studies. Although this was the first study using NIPPV as a primary ventilatory mode for treatment of RDS, there are limitations because the infants in this study were larger and more mature than the control infants. This apparent effect must require careful evaluation in a larger cohort.
New Modalities in Invasive Ventilation
1. Issues in Conventional Pressure-Targeted Ventilation
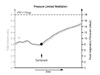
The pressure-targeted ventilation includes traditional time-cycled pressure-limited ventilation (TCPLV), flow-cycled pressure-limited ventilation, pressure control ventilation (PCV) and pressure support ventilation (PSV). Commonly all of these have a fixed pressure limit that the ventilator will not exceed (Fig. 1). TCPLV remains the most common approach for treatment of respiratory failure in the NICU worldwide.7 However, the delivery of tidal volume depends primarily on the patient's lung compliance. Thus, at a given pressure, tidal volume delivery will be lower when the lungs are stiff, and when compliance improves, the same amount of pressure will deliver a larger tidal volume (Fig. 2). This has implications for clinical practice, as there is a potential for overdistension of the lungs in the face of improving compliance especially in infants with RDS after surfactant therapy. This requires clinical decision making and ventilatory adjustment either manually or by using a computer-controlled algorithm as in some ventilators. Another distinguishing feature between different types of pressure-limited modalities is how the gas flow is delivered to the lungs. For example, in TCPLV inspiratory time and flow rates are fixed and chosen by the clinician. In contrast, flow-cycling results in variable inspiratory time (controlled by the patient). PCV and PSV also have variable inspiratory gas flow, which is proportional to patient effort.
2. Volume-Targeted Ventilation
Volume-targeted ventilation is a term that encompasses several modalities of breath delivery aimed at maintaining a target mechanical tidal volume by adjustments to the pressure and/or the inspiratory time.17 With this form of ventilation, the aimed tidal volume is set irrespectively of the state of lung compliance (Fig. 1A). The machine automatically adjusts the pressure to deliver the set tidal volume. Therefore, in stiff lungs, a higher pressure will be generated, and as lung compliance improves, the same tidal volume is delivered by auto-weaning of pressure. Thus, an advantage of volume-controlled ventilation compared to pressure-limited ventilation is that it responds to changes in lung compliance. However, these modalities may vary according to differences in volume parameter, whether the volume is measured by the ventilator to the circuit and patient or the actual VT, and whether this is during inspiration or exhalation. These also vary with regard to timing of the pressure adjustment. Some are instantaneous as volume is delivered, while others are based on prior breaths' measurements.
3. Hybrid Forms of Mechanical Ventilation
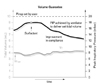
Attempts have been made to combine the desirable features of both pressure-targeted and volume-controlled ventilation resulting in a number of hybrid modalities. 18-22 These include volume guarantee (VG), pressure regulated volume control (PRVC), and volume assured pressure support (VAPS). VG and PRVC are primarily pressure-targeted modes of ventilation but involve computerized servo-controlled ventilation, in which the ventilator has an algorithm that adjusts the rise and fall of pressure to produce tidal volume delivery based on the previous breaths (Fig. 3). Volume guarantee ventilation is available on Draeger Babylog® 8000 ventilators and PRVC is available on the Servo 300A and the Servo-i® ventilators (Maquet). Both are forms of closed loop ventilation in which pressure is adjusted according to VT delivered. VG employs tidal volume measurements in a feedback loop to adjust the plateau pressure.23-25 The adjustments are based on the measured expiratory tidal volume of the previous breath. PRVC is a mode that initially delivers a test volume. Respiratory system compliance is then calculated based on the measured change in airway pressure. It is used to estimate the required plateau pressure to reach the target tidal volume. A breath-by-breath adjusted plateau pressure is subsequently delivered. The inspiratory flow pattern is decelerating. The inspiratory time is operator-set.
On the other hand, VAPS makes intra-breath adjustment of pressure and/or inspiratory time, until the desired volume has been delivered. This modality delivers a set inspiratory pressure plateau. In addition, tidal volume is measured within each breath. If it does not reach the target towards the end of inspiration, volume is supplemented by the device. If the targeted tidal volume is not achieved, the breath changes to a volume-controlled breath with a constant flow waveform and inspiration is continued until the set tidal volume is delivered. This mode is available on the VIP Bird Gold® infant/ pediatric ventilator.
New modes of Neonatal Ventilation
1. Patient Triggered Ventilation
Patient-triggered (or synchronized) ventilation initiates artificial breath by a patient-derived signal. The signal is a surrogate of spontaneous breathing and consists of a change such as airway flow or pressure, abdominal movement, or thoracic impedance.
This mode of ventilation includes synchronized intermittent mandatory ventilation (SIMV), assist/control (A/C) ventilation and Pressure support ventilation (PSV).26
In SIMV, the assist breaths occur only during windows of time established by manufacturer and set by the clinician and are delivered at the rate set by the operator if the patient effort is inadequate or absent. Between the mechanical breaths, the spontaneous patient-breath is supported only by the baseline pressure (PEEP) (Fig. 4A).27, 28
In A/C ventilation, mechanical breaths are patient-initiated if the patient's effort exceeds the trigger threshold, or ventilator-delivered if the patient is unable to trigger the ventilator or fails to breathe above the control rate. If the patient is consistently breathing above the control rate, lowering the control rate has no effect on the mechanical rate. An advantage of A/C over SIMV is that it supports every breath that meets the trigger threshold, thereby providing adequate minute ventilation at the minimal work of breathing. A/C can be either time- or flow-cycled, but only the latter produces both inspiratory and expiratory synchrony. Flow-cycling terminates inspiration at a percentage of peak flow rather than time.
PSV utilizes flow-cycling to achieve total synchrony as in flow-cycled A/C, but in addition it has variable inspiratory flow to enhance synchrony, comfort, and endurance.29, 30
PSV provides an inspiratory pressure 'boost' to spontaneous breaths to help overcome the work of breathing imposed by the narrow lumen endotracheal tube and ventilator circuit dead space(Fig. 4B). PSV was designed to support spontaneous breathing during weaning from mechanical ventilation. Although it resembles flow-cycled A/C, PSV does not have a control rate and is often used in conjunction with SIMV as a back-up maneuver until reliable respiratory drive is observed.31
2. Proportional Assist Ventilation
Proportional assist ventilation (PAV) is an adaptive form of mechanical ventilation in which the inspiratory pressure is determined by the elastic and resistive properties of the lung.32 With proportional assist ventilation (PAV) the level of ventilatory support is proportional to patient effort. PAV is based on the use of combined elastive and resistive un-loading of respiratory musculature to achieve gas exchange at lower mean airway pressure than with other forms of conventional mechanical ventilation. Thus far there are a few published clinical trials of PAV with newborns.33, 34 The study evaluated PAV, A/C, and IMV in a crossover design study with 36 infants, weighing 600-1,200 g, with mild to moderate acute respiratory illness. The PAV in that study resulted in lower mean airway and transpulmonary pressures at an equivalent fraction of inspired oxygen and similar carbon dioxide removal rates.33 PAV was subsequently investigated in 22 chronically ventilator-dependent preterm infants (mean birth weight 705 g) in a cross-over study design with conventional patient- triggered ventilation (SIMV or A/C).34 Ventilator pressure was statistically significantly lower during PAV compared with the conventional triggered control mode. The authors concluded that PAV safely maintains gas exchange at lower mean airway pressures compared with PTV without adverse effects, however backup conventional ventilation breaths must be provided to prevent apnea-related desaturations.34
A gain control for the volume-proportional assist ventilation allows the clinician to set the ratio of delivered ventilator pressure per unit of tidal volume in cm H2O/mL on a continuous scale.32 A separate control sets the gain for flow-proportional assist. Flow-proportional assistance delivers ventilator pressure waveforms in proportion to tidal airflow rate (cm H2O/L/s).32 If this feature is activated during both inspiration and expiration (full-cycle resistive unloading), it will facilitate exhalation, shorten the expiratory time constant, and help to avoid inadvertent PEEP in infants with a high airway resistance.
An alternative drive of proportional amplification is the electrical activity of the diaphragm.35 Neurally adjusted ventilatory assist (NAVA) is a mode of assisted mechanical ventilation that uses the electrical activity of the crural diaphragm (EAdi) to control the ventilator. (Fig. 5) It is assumed that the electrical activity of the crural diaphragm is an indicator of the global inspiratory muscle activity during breathing. The raw EAdi is obtained from an array of electrodes attached to a nasogastric tube and placed in the lower oesophagus (Fig. 6A). The phasic EAdi triggers the ventilator at initial inspiration, drives the delivery of inflation pressure in proportion to the rising EAdi during the inspiratory effort, and cycles off the ventilator pressure at end of inspiration. The magnitude of the inspiratory assist is operator adjustable by setting a proportionality constant, called 'NAVA gain' (Fig. 6B). It determines the increase in ventilator pressure per unit of rise in EAdi during inspiration. NAVA maintained respiratory gas exchange and synchronous ventilator pressure delivery through nasal prongs in rabbits with acute lung injury when there was a large air leak at the ventilator-airway interface.36 Recent clinical studies in low birth weight infants revealed NAVA can improve patient-ventilator interaction, even in the presence of large leaks.37
Conclusions
The target of neonatal ventilation therapy is to improve pulmonary gas change and reduce the lung injury. In that meaning, the ideal mode is the one that provides adequate and consist tidal volume delivery and minute ventilation at low air pressure. Nowadays, new ventilators have a variety of modes and modalities. For the clinician, it is very important to understand the mechanism of these new functions of ventilators to make the appropriate choice of state-of-the-art ventilation therapy.




 XML Download
XML Download