

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Hypopharyngeal carcinoma is a very aggressive cancer that is generally diagnosed at advanced stages and consequently has a poor prognosis and low survival rate. The treatment of these tumors is designed to cure the patient with the cancer and to preserve or restore physiologic function of the laryngo-pharyngeal complex as well. However, the need for extensive ablative surgery often coupled with radiation therapy renders many patients incapable of performing the basic human functions of swallowing and speech. Loss of such integral functions has a dramatically negative influence on the patients' quality of life, which has already been threatened by the aggressive nature of this disease. Therefore, it is imperative to use a reliable surgical strategy with low morbidity that will allow expedient restoration of speech and swallowing. Consequently, conservation surgery for hypopharynx carcinoma offers a wider resection with promising functional results in hypopharyngeal cancer patients. Recently several procedures were introduced for this purpose and we review the introduction and indications of those conservation methods in hypopharyngeal cancer surgery.
Figures and Tables
Fig. 1
Partial pharyngectomy via the lateral pharyngotomy. (A) Area removed, including the posterolateral hypopharyngeal wall and a portion of the thyroid ala. (B) Dotted lines show cuts on the thyroid cartilage, hyoid, and vallecula. (C) After entry into the hypopharynx, the specimen is reflected laterally and final cuts are made. (D) Defect following excision of the posterolateral hypopharyngeal tumor.

Fig. 2-1
Case of partial pharyngectomy via lateral pharyngotomy. Right lateral wall of the hypopharynx cancer (star).
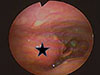


Fig. 3
Partial Laryngopharyngectomy. (A) The resection margin after a partial laryngopharyngectomy for a medial pyriform tumor is shown in the superior view. (B) This view demonstrates the bone and cartilage cuts for a partial laryngopharyngectomy. (C) The completed resection of the medial pyriform tumor is shown. The epiglottis may be divided (as described in the text) or removed completely as shown here. (D) With resection of the arytenoid, the ipsilateral true vocal cord must be sutured in the midline to the cricoid to prevent aspiration. The laryngeal mucosa is reapproximated as much as possible as shown.

Fig. 4
Wide Vertical Hemipharyngolaryngectomy. Top left. Vertical section of the epiglottis. A, B=two parts of epiglottis; C=thyroid cartilage; D=cricothyroid membrane; E=cricoids cartilage. Top right. Section through the inetrarytenoid space and subperichondrial dissection of the cricoids cartilage until the cricoarytenoid joint. A=right vocal cord; B=right hemiepiflottis; C=left arytenoid cartilage; D=left hemiglottis; E=cricoids cartilage; F=left vocal cord. Bottom left. Fixation of the tendon through the two drilled holes and the suture of the skin around the tendon to create a new glottis plane. A=remaining vocal cord; B=anterior fixation of tendon; C=anterior suture between the flap and the subglottic mucosa; D=cricoid cartilage; E=new glottic plane; F=radial vascular pedicle; G=cutaneous sensitive branch. Bottom right. Progressive suture between the borders of the flap and the neighboring structures, creating a new pyriform sinus. A=anterior fixation with the perichondrium of the thyroid cartilage; B, C=inferior fixation to the cricoid cartilage; D=posterior fixation to the pharyngeal mucosa.





References
1. Muir C, Weiland L. Upper aerodigestive tract cancers. Cancer. 1995; 75:1 Suppl. 147–153.

2. Hussey DH, Latourette HB, Panje WR. Head and neck cancer: an analysis of the incidence, patterns of treatment, and survival at the University of Iowa. Ann Otol Rhinol Laryngol Suppl. 1991; 152:2–16.
3. Driscoll WG, Nagorsky MJ, Cantrell RW, Johns ME. Carcinoma of the pyriform sinus: analysis of 102 cases. Laryngoscope. 1983; 93:556–560.
4. Bataini JP, Bernier J, Brugere J, Jaulerry C, Picco C, Brunin F. Natural history of neck disease in patients with squamous cell carcinoma of oropharynx and pharyngolarynx. Radiother Oncol. 1985; 3:245–255.
5. Scharpf J, Esclamado RM. Reconstruction with radial forearm flaps after ablative surgery for hypopharyngeal cancer. Head Neck. 2003; 25:261–266.
6. Seidenberg B, Rosenak S, Hurwitt ES, Som ML. Immediate reconstruction of the cervical esophagus by a revascularized isolated jejunal segment. Ann Surg. 1959; 149:162–171.
7. Harii K, Ebihara S, Ono I, Saito H, Terui S, Takato T. Pharyngoesophageal reconstruction using a fabricated forearm free flap. Plast Reconstr Surg. 1985; 75:463–474.
8. Gilbert RW, Neligan PC. Microsurgical laryngotracheal reconstruction. Clin Plast Surg. 2005; 32:293–301.
9. Plouin-Gaudon I, Lengelé B, Desuter G, Rombaux P, Ledeghen S, Grégoire V, Hamoir M. Conservation laryngeal surgery for selected pyriform sinus cancer. Eur J Surg Oncol. 2004; 30:1123–1130.
10. Kelly KE, Anthony JP, Singer M. Pharyngoesophageal reconstruction using the radial forearm fasciocutaneous free flap: preliminary results. Otolaryngol Head Neck Surg. 1994; 111:16–24.
11. Disa JJ, Pusic AL, Hidalgo DA, Cordeiro PG. Microvascular reconstructionof the hypopharynx: defect classification, treatment algorithm, and functional outcome based on 165 consecutive cases. Plast Reconstr Surg. 2003; 111:652–660.
12. Stark B, Nathanson A. The free radial forearm flap: a reliable method for reconstruction of the laryngohypopharynx after in-continuity resection. Acta Otolaryngol. 1998; 118:419–422.
13. Urken ML, Blackwell K, Biller HF. Reconstruction of the laryngopharynx after hemicricoid/hemithyroid cartilage resection. Preliminary functional results. Arch Otolaryngol Head Neck Surg. 1997; 123:1213–1222.
14. Delaere PR, Liu Z, Feenstra L. Tracheal autograft revascularization and transplantation. Arch Otolaryngol Head Neck Surg. 1994; 120:1130–1136.
15. Delaere PR, Blondeel PN, Hermans R, Guelinckx PJ, Feenstra L. Use of a composite fascial carrier for laryngotracheal reconstruction. Ann Otol Rhinol Laryngol. 1997; 106:175–181.
16. Nakatsuka T, Harii K, Ueda K, et al. Preservation of the larynx after resection of a carcinoma of the posterior wall of the hypopharynx, versatility of a free flap patch graft. Head Neck. 1997; 19:137–142.
17. Scharpf J, Esclamado RM. Analysis of recurrence and survival after hypopharyngeal ablative surgery with radial forearm free flap reconstruction. Laryngoscope. 2005; 115:429–432.
18. Chantrain G, Deraemaecker R, Andry G, Dor P. Wide vertical hemipharyngolaryngectomy with immediate glottic and pharyngeal reconstruction using a radial forearm free flap: preliminary results. Laryngoscope. 1991; 101:869–875.
19. Chantrain G, Deraemaecker R. Glottic reconstruction after cricohyoidoepiglottopexy with a radial forearm free flap that includes the tendon of the palmaris longus: preliminary results and perspectives. Laryngoscope. 1994; 104:1035–1040.
 XML Download
XML Download