

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Scissors-bite is characterized by a labial eruption of the upper molar and/or lingual tipping of the lower molar and is caused by an arch-length discrepancy in the posterior region.1 Mandibular transverse skeletal deficiencies are common clinical problems associated with narrow basal and dentoalveolar bones.2 Scissors-bite of several molars resulting from a transverse skeletal deficiency is called a Brodie bite.3 Buccal crossbite has traditionally been treated by extraction, dental arch compensations, or orthognathic surgery.4 Mandibular widening by distraction osteogenesis (DO) was introduced as an alternative treatment for scissors-bite.4 DO is the biologic process of new bone formation between bone segments that are gradually separated by incremental traction.5 In mandibular symphyseal distraction osteogenesis (MSDO), an osteotomy is performed after which the healing callus is gradually stretched. Ilizarov's principles are applied, including the need for a latency period, rhythm and amount of traction, consolidation period, and the rigidity of the distractor during distraction.4
The purpose of this case report is to provide a description of the treatment of a unilateral buccal crossbite with MSDO that included a tooth-supported distractor and cross elastics.
DIAGNOSIS AND ETIOLOGY
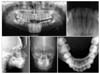
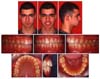
The patient was a 14-year-old boy with posterior buccal crossbite (Fig 1). He was referred by his family dentist for orthodontic consultation. His medical history revealed nothing remarkable. The patient had a normal growth pattern. Examination of the patient revealed an asymmetric face, a normal lower facial height, and a convex profile. Intraoral examination showed a Class I molar relationship on the left side and a buccal crossbite on the right side. The maxillary right first molar had not overerupted. All permanent teeth had erupted except the third molars. Oral hygiene was satisfactory, and no periodontal problems were visible. There was no lateral shift between the centric relation and centric occlusion. It was concluded that the patient had a true unilateral buccal crossbite on the right side.
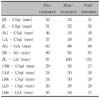
There was a discrepancy in the maxillary arch length of 1 mm and discrepancy in the mandibular arch length of -3 mm. The maxillary dental midline was normal, but the mandibular midline was 1.5 mm to the left of the maxillary dental midline. The pretreatment lateral cephalometric radiograph measurements showed optimal values (Table 1). The pretreatment posteroanterior cephalometric radiograph indicated that the width of the maxilla was normal, as determined by the interjugal distance. However, measurements at the biantegonion showed a severe mandibular transverse deficiency (Table 2). The transverse mandibular skeletal deficiency and mandibular asymmetry were the primary causes of the scissors-bite (Fig 2).
TREATMENT OBJECTIVES
The treatment objectives for the patient were as follows. The buccal nonocclusion, facial asymmetry, and midline shift should be corrected. Mandibular molars and the premolars should be made upright. The class I molar canine relationship should be maintained on the left side and established on the right side. Other orthodontic problems of the patient can be solved by fixed orthodontic treatment.
TREATMENT ALTERNATIVES
Traditional approaches such as Schwarz devices,6 or functional devices,7 extractions, dental tipping, or mandibular arch expansion could resolve the transverse mandibular deficiency. Lip bumpers, Schwarz devices, or functional devices are commonly used to treat transverse mandibular deficiency in growing patients. However, mandibular arch expansion in older patients or expansion in the anterior area is unstable and tends to relapse toward the original dimension.8 Dental expansion is unpredictable and could result in relapse and undesirable side effects.9
Unilateral mandibular widening with MSDO is another alternative for treating mandibular transverse deficiency. With this technique, bone segments are gradually separated and expansion occurs not only in the dental and skeletal structures, but also in soft tissues such as the masticator muscles, subcutaneous tissue, and skin, which minimizes the chance of relapse.10
TREATMENT PROGRESS
Preadjusted straight-wire mechanics (0.022 slot MBT) were used. A 0.016-inch nickel-titanium arch wire was placed in the upper arch. After leveling and alignment, a 0.019 × 0.025-inch stainless steel arch wire was adjusted to fit the maxillary arch to provide reinforcement anchorage during unilateral expansion of the mandible. A 0.014-inch Australian arch wire was placed in the lower arch. Second-order bends were placed in the wires to separate the roots of the mandibular central incisors. The tooth-supported distractor was fabricated from a hyrax screw (Fig 3) and was adjusted to the lower first premolars and the lower first molars.
A midsymphyseal osteotomy was performed under general anesthesia. A horizontal incision was made 5 to 7 mm labial to the depth of the vestibular sulcus, from canine to canine, and the muscle was reflected.2 The soft tissue above the incision was carefully elevated between the central incisors to provide access for the superior portion of the osteotomy.2 The inferior portion of the mental symphysis was sectioned vertically with a reciprocating saw.2 A small interdental osteotome was used, and a light tapping pressure was applied to complete the interdental osteotomy between the root tips of the central incisors, taking care to avoid injuring the teeth.2 Immediately after the osteotomy, the appliance was tested for expansion. After a 1-week latency period, the distraction process was started by making four turns per day, two in the morning and two at night, which expanded the mandible 0.8 mm per day (Fig 4). The patient was instructed how to place the intermaxillary cross elastics from the upper right side to the lower left side. During the distraction period, the patient wore the cross elastics full time to provide more transverse widening on the right side than the left side. The distraction was stopped at the end of day 11, and the mandible had been widened approximately 9 mm. At the end of the 3-month consolidation period, the appliance was removed and a lingual arch was placed on the lower arch. A 0.014-inch nickel-titanium arch wire was placed in the lower dental arch (Fig 5). The mandibular second molars were added to the system and made upright. The retention was provided by an upper Hawley retainer and lower fixed lingual retainer. The patient was controlled for 1 year after the end of the treatment. Clinical examination andradiographic and model analysis showed that the treatment results remained stable.
RESULTS
Facial asymmetry and scissors-bite were successfully corrected by the end of treatment (Fig 6). The posterior unilateral buccal crossbite was eliminated, and optimal posterior occlusion was achieved. The mandibular intercanine and intermolar width increased during MSDO and fixed orthodontic treatment (Fig 7). Dental model analysis showed that intercanine width increased from 22.57 mm to 24.74 mm, and the intermolar width increased from 32.33 mm to 40.72 mm. During the retention period, intermolar width decreased to 40.07 mm. The distance between the right antegonion and the midsagittal plane increased from 46 mm to 50 mm. The distance between the left antegonion and the midsagittal plane increased from 37 mm to 39 mm (Table 2). The distance between the lower right molar and the midsagittal increased from 24 mm to 30 mm. The distance between the lower left molar and the midsagittal plane increased from 26 mm to 28 mm (Table 2). Asymmetric widening of the mandible was achieved with the use of cross elastics. The transverse occlusal plane was canted counterclockwise, which is possibly also due to using intermaxillary cross elastics. At the end of the treatment period, no significant lateral cephalometric changes were observed. Treatment produced a notable change in facial symmetry and balance (Fig 8).
DISCUSSION
Mandibular arch expansion has been attempted with a variety of methods such as Schwarz devices, lingual arches, functional appliances, and arch wires. These methods tend to produce only limited dimensional change, and the long-term stability is questionable.11 If arch length deficiency correction by an expansion of the mandibular bone is desired, MSDO can be performed to increase the dimension of the innate mandibular basal bone. Advantages of DO are greater predictability, more physiologic improvements, and better stability.12 By the end of treatment in the present case, the mandibular bone was successfully expanded.
Although MSDO has several advantages, the surgeon must be careful because removing excess osseous tissue or injuring the periodontal ligament could cause periodontal defects or ankylosis of the involved teeth.13 The risk of damaging the root during the surgery is relatively low when the roots of the incisor are separated during the initial treatment phase.12 When there is not adequate space for alignment but sufficient inter-radicular space presents parasagittally, a stepwise parasagittal osteotomy is recommended.13 In the present case, roots of the mandibular incisors were carefully separated using second-order bends, so damage was prevented. In addition, MSDO can cause phonetic problems and temporomandibular joint (TMJ) disorders, and can expose the patient to periodontal infection.14
Cope et al.15 reported that moving teeth into newly distracted bone accelerates the maturation process of new bone. Thus, orthodontic tooth movement increased bone volume at the distraction site. Mommaerts et al.16 suggested that as long as the tooth apices are not damaged during osteotomy, periodontal and dental morbidity is transient and limited to the distraction and consolidation period. In the present case, tooth movement into the distraction region was initiated after the consolidation period. During the entire treatment phase and follow-up period, the patient had a healthy periodontal pocket depth in the lower incisors and exhibited no gingival recession in the distraction region.
Some researchers have suggested that MSDO may lead to TMJ alterations and symptoms. For example, Stelnicki et al.17 reported that mandibular distraction in the transverse dimension produces severe degenerative changes that do not disappear at the end of the 8-week consolidation period. However, a histologic study by Bell et al.18 demonstrated that change in the condyle after MSDO is minor, and Mommaerts et al.16 reported that moderate symphyseal expansion will not cause clinical problems in the TMJ area. Our patient experienced no clicking sounds or TMJ pain during treatment or follow-up.
MSDO devices are classified as intraoral or extraoral.19 Intraoral devices are commonly used for esthetic reasons and can be tooth-borne, bone-borne, or hybrid.4 Each appliance has advantages and disadvantages. It is thought that tooth-borne distractors produce greater dentoalveolar expansion than bone-borne distractors.19 If the patient needs buccal uprighting of the mandibular posterior teeth, tooth-borne devices may be more useful. The crossbite in the present case appeared to be a skeletal transverse problem with genetic origin. However, slight tipping of the mandibular right posterior teeth may have contributed to the unilateral scissors-bite. The tooth-supported distractor was adjusted to the lower first premolars and lower first molars, and buccal uprighting of the posterior mandibular teeth was achieved by the end of treatment.
In this case, the facial asymmetry and posterior unilateral buccal crossbite were eliminated. The mandibular intercanine and intermolar width increased during the MSDO and fixed orthodontic treatment. The dental model measurements showed that intercanine width increased from 22.57 mm to 24.74 mm, and intermolar width increased from 32.33 mm to 40.72 mm. During the retention period, intermolar width decreased to 40.07 mm (Fig 9). The distance between the right antegonion and midsagittal plane increased 4 mm, and the distance between the left antegonion and midsagittal plane increased 2 mm (Table 2). The distance between the lower right molar and the midsagittal plane increased 6 mm and the distance between the lower left molar and the midsagittal plane increased 2 mm (Table 2). These increases were the result of the skeletal expansion and dental arch expansion. The skeletal expansion achieved with MSDO was especially important for correcting the facial asymmetry. The dental arch expansion was achieved by MSDO and fixed orthodontic treatment. This tooth-supported distractor provided the dental arch expansion, and cross elastics produced the asymmetric widening of the mandible. The transverse occlusal plane was canted counterclockwise, which may have been also due to using intermaxillary cross elastics.
Generally, MSDO increases the width of the anterior region of the mandible more than the posterior region. However, dental measurements of our patient revealed greater widening in the mandibular first molars than in the mandibular canines. This result can be explained by post-distraction orthodontic treatment, which aligned the arch, closed dental spaces, and resolved dental crowding by moving anterior teeth into newly formed bone in the distraction gap, as described by Del Santo et al.20 Most of the expanded space was used to correct crowding.
With the interarch cross elastics, the right mandibular arch was expanded more than the left side during the distraction period. During the elastic usage period, a thick and rigid arch wire was seated to the maxillary arch to prevent extrusion of the right upper molars. The occlusal plane canted counter clockwise, as shown by anteroposterior cephalometric superim-positions. The right segment of the maxillary arch protruded slightly, and the right segment of the mandible was expanded. Therefore, the mandibular skeletal asymmetry was corrected.
CONCLUSION
Mandibular skeletal widening was achieved with MSDO, and dental arch widening of the mandible was achieved by MSDO and fixed orthodontic treatment. The right side of the mandible was expanded more than the left side by using interarch cross elastics. Thus, unilateral scissors-bite can be treated successfully through unilateral widening of the mandible by MSDO with interarch cross elastics and fixed orthodontic treatment (Fig 10). This procedure proved to be effective for buccal crossbite in a patient with a mandibular skeletal transverse deficiency that included narrow basal and dentoalveolar bones, leading to stable treatment results.









 XML Download
XML Download