

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Clinical decision making in orthodontics depends primarily on detecting departures from defined norms, which are available as various standardized indices.1 However, subjective psychosocial perceptions play an important role in orthodontics, and treatment might be more influenced by demand than by need,2 because the patient receiving treatment should be satisfied by the improved function and aesthetics. Therefore, the importance of patients' perceptions regarding orthodontic treatment cannot be underestimated.3
While treatment demand is affected by perceived need and cost,4,5 patients' concerns do not always coincide with professional assessments of their treatment need.1,3,6 Controversial and diverse associations have been observed between self-perceived and normative treatment needs,2,5-9 ranging from moderate2,10 to weak.3,11,12 However, no correlations have exceeded 60%, and there is a consensus that normative findings often indicate higher treatment needs than do perceived needs.1,2 The distinction between perceived and treatment needs has clear service-related implications, because the treatment need is usually determined by clinical examination.1 The associations are of interest to orthodontists because they help establish relevant methods to assess treatment priority when selecting orthodontic patients in a publicly funded oral health care system;2 moreover, the success of care should be assessed on the basis of whether it meets the expectations of both patients and clinicians.13
Self-perception of body image may change with age.14,15 Some studies suggest that young adults may have higher expectations than children,4,11,15-18 whereas others have found a lower willingness toward treatment in young adults.14,16 There are also indications that younger participants might have appropriate self-concepts similar to those of older participants.10,19,20 These imply that findings of studies on children cannot be generalized to young adults and indicate the need for such studies in the latter group. However, only a few studies have assessed the correlations between normative findings and self-perceived needs among young adults,11,13,14 and 2 of these enrolled less numbers of participants.11,14 The aim of this study was to evaluate the associations between a developed self-evaluation questionnaire (SEQ) and components of the index of orthodontic treatment need (IOTN),21,22 including the dental health component (DHC), aesthetic component (AC), and the AC determined by the examiner (ACE)23 in a sample of 18- to 22-year-old Iranian walk-in dental patients, during 2007 - 2008.
MATERIAL AND METHODS
On the basis of a pilot study, the sample size of this descriptive cross-sectional study was predetermined to be 240 participants (120 men and 120 women) to obtain a test power of 0.84. The participants were selected via the cluster sampling method from 6 government dental clinics in 6 different administrative residential districts of Shiraz, Iran (40 patients from each district). The inclusion criteria were as follows: the presence of full permanent dentition excluding the third molars, the absence of any orthodontic treatment history, and age between 18 and 22 years. The ethics of the study were approved by the research committee of the Shiraz University of Medical Sciences.
IOTN-DHC
After obtaining informed consents, the IOTN-DHC was assessed clinically under the light of a dental unit, by a dentist who had been trained by one of the authors (H. P.). Scores 1 and 2 indicated no treatment need, score 3 indicated a moderate need, and scores 4 and 5 indicated a definite need for treatment.
IOTN-AC and IOTN-ACE
The patients were asked to select 1 of 10 colored photographs of the IOTN-AC which they felt most resembling their dental attractiveness (on a scale of 1 to 10), regardless of technical details such as open bite or class III malocclusion that were not present in the photographs. These images represented a range of dental appearances from the extremes of desirability to unattractiveness. The examiner also matched an IOTN-AC image for each participant (the IOTN-ACE). The AC images 1 to 4, 5 to 7, and 8 to 10 were assigned to the categories "no treatment need," "moderate need," and "definite need," respectively.
SEQ
The SEQ consisted of more than 100 questions, partly borrowed from other studies,8,10,14,17,19 and was evaluated by 3 orthodontists and 2 psychologists. It consisted of eleven 5-point Likert scale questions with answers representing a range between 0 ("not at all") and 4 ("certainly") (Table 1). A pilot study of 60 patients confirmed the high internal consistency of the questionnaire scores (Cronbach's α = 0.88). The mean scores of the questionnaires were calculated. Rounded mean questionnaire scores of 0 and 4 were regarded as "no perceived treatment need" and "definite treatment need," respectively, and rounded mean scores of 1, 2, and 3 represented low, moderate, and high treatment needs, respectively.
The patients also selected the most pressing complaints from the following options derived from the most frequent complaints observed in the pilot study: (0) No orthodontic complaints, (1) crowding, (2) protruded upper incisors, (3) gummy smile, (4) occlusal interferences, and (5) diastema.
RESULTS
The mean age of the patients was 20.37 ± 1.37 years. Within the group, 12.9% were aged 18 years, 15.8% were aged 19 years, 18.8% were aged 20 years, 25.8% were aged 21 years, and 26.7% were 22 years. According to Cohen's Kappa, the reliability of the interexaminer findings, the main examiner's scores, and the patients' IOTN-ACE scores were 75%, 84%, and 80%, respectively (p < 0.001).
Figs 1, 2, 3, 4 illustrate the distribution of treatment needs, established using the evaluation methods employed. The average of all question scores in the SEQs (n = 240 × 11) was 0.900 (Table 1). The proportions of participants who selected chief complaint values were 27.7% for 0, 38.7% for 1, 12.8% for 2, 6.4% for 3, 4.3% for 4, and 10.2% for 5. The proportions of the IOTN-AC categories "no treatment need," "moderate need," and "extreme need" were 93.2%, 5.6%, and 1.3%, respectively (Fig 3), whereas the proportions of the IOTN-ACE categories were 92.7%, 3.9%, and 3.4%, respectively (Fig 4).
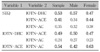
According to Spearman's correlation coefficient, the scores of all of the evaluation methods were significantly correlated with each other (all p values ≤ 0.001; Table 2). Age, gender, and the patients' chief complaints were not significantly associated with the results of any of the methods of assessing treatment need (Table 3).
The chi-square test showed that the score proportions of the IOTN-DHC and the SEQ differed significantly in distribution patterns (p = 0.01. The distribution of score proportions of the IOTN-AC and the IOTN-ACE were not significantly different (p = 0.086).
DISCUSSION
Among the methods used, the IOTN-ACE had moderate correlations with each of the other methods, whereas the IOTN-AC was moderately correlated only with the IOTN-ACE, which, not surprisingly, was the greatest correlation. The correlation between the IOTN-DHC and the self-evaluation approach was the second highest.
Self-evaluation
The patients' chief complaints in this study were not associated with their normative or self-perceived orthodontic needs; this may point to the need for more comprehensive examinations rather than relying on the chief complaint. The observed discrepancy between the results of the SEQ and the IOTN-DHC might be attributed to the patients' attitudes and expectations, and in some cases, to the need for prosthodontic treatments rather than orthodontic treatments. The "high treatment need" group of the IOTN-DHC consisted of malocclusions in areas the patient might be unaware of, as was confirmed by the comparison of the IOTN-DHC and the IOTN-AC.2 On the other hand, certain malocclusions critical to the patient might be considered normal according to the IOTN-DHC, or even be omitted from its criteria. These include gingival appearance and the presence of interdental spaces, which are considered important in some patients' opinions. Some authors authors have reported a poor correlation between the IOTN-DHC scores and participants' self-evaluation (e.g., 19%2 or 7 - 14%),3 whereas the results of others were in harmony with the correlation observed in this study (53%).8 The questionnaire presented in this study eclipsed the normative needs comparatively well. The correlation between the results of the SEQ and the IOTN-AC in our study (35%) was similar to that reported in other studies (47%,2 34%,8 31%,16 and 28 - 39%3).
As reported by Phillips and Beal,9 the correlation between the SEQ and the IOTN-AC was not meaningful (rho < 0.4). The IOTN-AC represents self-perceived severity of the malocclusion,9 whereas the questionnaire included items related to positive feelings towards self, and not only dental appearance. This correlation also implied a high need for aesthetic improvements among the subjects despite their proper dental appearance. The finding was in contrast to that of a Finnish study in which most of the participants were not meant to receive orthodontic treatments despite their comparatively low satisfaction with their oral appearances.13 Apparently, the Finnish health care system places more emphasis on the functional aspects rather than on aesthetics.13,24 Moreover, a rather lower level of satisfaction could be expected since more than one-third of the treated Finnish adolescents still showed diastema and crowding afterwards.13 The IOTN-ACE showed a meaningful correlation with selfperceived needs in this study, indicating that its reliability was higher than that of the AC.
IOTN
The slightly lower correlation between the IOTN-DHC and the IOTN-AC found in this study as compared to that reported in another study3 might be because of differences in ethnic backgrounds and psychosocial needs. The scores of the IOTN-AC and the IOTN-ACE were inclined to the attractive end. A similar pattern was observed in several other studies,2,16,23 but some studies showed an evenly distributed AC histogram,25 or even an inclination to the unattractive end.3 The "no treatment need" scores of the AC might be redefined as "AC images 1 and 2" to make them more consistent with the DHC or self-evaluation.13 Furthermore, a modified version of the IOTN-AC with more images on the attractive end might be advantageous for evaluating self-perception towards dental appearance with higher accuracy. Throughout this study, the IOTN-AC scores were slightly closer to the attractive end than were the scores of the IOTN-ACE; this finding was similar to that of other studies.2,8 This might be attributed to the dentists' better knowledge of dental appearance as well as to the difficulties young adults may have in assessing their dental appearance;1,7,13 such a difference might increase if the examiner was an orthodontist.8
Age and gender
While men may show higher normative needs, the genders do not differ in perceived needs.2 In this study, the need for orthodontic treatment was slightly, but insignificantly, lower in men than in women. This finding was supported by those of previous studies,8,19,20 but opposed by others that reported a significant difference between the genders.2,16,17 The age, race, level of expectations (probably affected by their culture), and socioeconomic status of each population might contribute to the controversy. The participants' age did not correlate to their self-evaluation. This was in contrast to the findings of some other studies.13,16 Moreover, the consciousness regarding self-image might be more prominent during adolescence.15 Therefore, most of these patients might have had an appropriate self-evaluation method.
Limitations
The present study might be limited by some factors. In this study, the subjects were selected from dental clinics that were not necessarily the most representative of the local population, as dental patients might have a better insight towards their dental condition or appearance. Social background, which could influence orthodontic treatment needs (i.e., dental attractiveness),2,15,17,18 was not assessed in this study. The IOTN-AC is composed of 10 photographs of 12-year-old children, which might affect the reliability of AC images images selected by older patients.18 However, the correlation between the IOTN-AC and the IOTN-ACE might indicate an appropriate reliability.
The significant correlations found between the findings of the objective and subjective methods used in this study may indicate that self-perceived needs of young adults may moderately reflect their objective treatment need. However, because there was still a considerable difference between these, a treatment plan should address both the self-perceived and the normative needs.
CONCLUSION
Within the limitations of this study, there were positive and significant weak-to-moderate correlations between the components of the IOTN and young-adult patients' self-evaluation results.
The association found between the IOTN and self-evaluation in young adults was similar to that observed in children.
The IOTN-ACE seemed to be more reliable than the IOTN-AC in young adults.
The age and gender and the chief complaint did not correlate to the normative or self-perceived treatment needs.






 XML Download
XML Download