

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tooth transposition, considered a subdivision of ectopic eruption, can be defined as the positional interchange of two adjacent teeth in the dental arch.1 Complete transposition refers to situations in which crowns and roots of the involved teeth exchange places in the dental arch, and incomplete transposition refers to stuations in which the crowns are transposed but the roots remain in their normal positions.2 The most accepted etiologic possibility is based on genetics.1,3-6 The orthodontic literature reveals that tooth transposition seems to occur more often unilaterally than bilaterally,1,7,8 with maxillary prevalance6,8 and no sex preference.9,10 The canine is one of the most commonly involved teeth in the transposition phenomenon. The canine shows the highest incidence of transposition, then the first premolar,11,12 less often with the lateral incisor,13-15 rarely with the central incisor16 and extremely rarely with the second premolar17 or the first molar.18
This case report presents the treatment of a female patient, who showed complete transposition of a maxillary canine and first premolar. The defect was corrected with the help of mini-implant anchorage without any reshaping procedures, including enamel reduction or restoration, in an acceptable treatment time period (24 months).
DIAGNOSIS AND ETIOLOGY
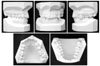
A female patient, aged 26 years, presented with transposition of the maxillary left canine and first premolar. The patient had a Class I skeletal pattern with good facial relationships and a slightly convex profile (Fig 1). A mild Class II dental malocclusion in the transposition side and Class I dental relationship in the right side were recorded. We also noted a 2-mm deviation of the maxillary midline towards the affected side. The arch length discrepancy was 4 mm in the maxillary and 6 mm in the mandibular dental arch (Figs 1 and 2). Radiographic examination revelaed complete transposition (Fig 3).
TREATMENT OBJECTIVES
We aimed to establish functional Class I molar-canine relationships and a satisfactory esthetic smile without extractions and without any reshaping procedures, including enamel reduction or restoration, in order to correct the transposition with the help of palatal mini screw anchorage. Further, we aimed to create an ideal overbite and overjet relationship while correcting mid-lines and root inclinations.
TREATMENT ALTERNATIVES
Treatment plans were based on the results of cephalometric and study model analyses. Facial appearance was satisfactory; therefore, extraction treatment was contraindicated. When deciding on a treatment plan of [Maxilla 4-3] transposition, the clinician should consider at least 2 options: aligning the involved teeth in their transposed positions or moving them to their correct anatomic position in the dental arch. Dental and facial esthetics of the maxillary anterior teeth should be carefully evaluated and considered when deciding which treatment option is suitable. A treatment plan involving the alignment of the teeth in their transposed positions and composite crown restoration for canine and premolars was offered but was declined by the patient.
TREATMENT PROGRESS
This case of complete transposition of the maxillary canine and premolar was treated with palatally located mini-implant anchorage and fixed orthodontic treatment mechanics. Esthetic and occlusal considerations suggested the alignment of the transposed teeth to their correct anatomic positions in the dental arch. The buccopalatal width of the bone is not sufficient to support 2 adjacent teeth that are moving in opposite directions. For this reason, mini-implant anchorage was used to move the transposed premolar in the palatal direction.
Treatment was initiated with leveling of the maxillary arch. After using superelastic leveling arches, a 0.016 × 0.022 inch rectangular stainless steel arch wire was placed. Then, the first premolar was moved palatally with the help of a palatal implant (Fig 4). Necessary space for canine placement was provided by mini-implant anchorage, and root interferences were prevented with a 0.016 × 0.022 inch stainless steel wire with an offset bend at the transposition region, maintaining the buccal position of the canine. Simultaneously, the maxillary canine was mesialized along a buccal path over the maxillary first premolar, directed by an active open coil spring between canine and second premolar over the 0.016 × 0.022 inch continuous stainless steel arch wire. After 14 months, following repositioning of the canine, a removable 0.032-inch TMA transpalatal arch with premolar extensions was inserted in the palatal sheath of the first molars. A unilaterally activated transpalatal arch was used to move the premolar labially, back to its normal position (Fig 5). Simultaneously, the mandibular arch was bonded. An open coil was placed between the maxillary right canine and second premolar to gain enough space for the first premolar and for midline correction.
Bite raising was achieved by bonding composite on the occlusal surfaces of both mandibular first molars. By 18 months, the maxillary left first premolar was included in the fixed mechanics. Special effort was made to achieve optimal torque of the teeth with a rectangular stainless steel arch wire. A second lower premolar bracket (Mini Ovation, Dentsply GAC International, Bohemia, NY, USA) of 0.22 inches with -22 torque degrees was placed upside down to achieve optimal torque control of the palatally displaced transposed premolar. For the transposed canine, another second lower premolar bracket (Mini Ovation, Dentsply GAC International, Bohemia, NY, USA) of 0.22 inches with -22 torque degrees was placed in order to achieve the necessary palatal root movement (Fig 6).
RESULTS
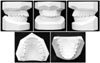
The total treatment time was 24 months, which although relatively long in general is yet acceptable considering the absolute correction achieved. The clinical result at the end of the treatment was satisfactory (Figs 7 and 8). The maxillary canine and first premolar were successfully positioned. Alignment was obtained, and intercuspation was adequate. Ideal overjet and overbite were also achieved. Class I dental relationships were established. Root parallelism was achieved.
Nevertheless, the maxillary canine exhibited facial recession, probably because it was initially positioned buccally. To maintain the level of the attached gingiva of the canine with the adjacent teeth, intrusion of the canine was avoided.
Supporting tissue was examined after treatment, and no alveolar bone damage was observed.
The amount of root and crown movements in this case was not favorable for the roots because of the occurrence of root resorption. Radiographic analysis showed moderate resorption of the canine roots in comparison to its controlateral (Fig 9). Using palatal mini-implant anchorage involves less treatment time when compared to orthodontic procedures alone. At the 2-year follow-up, the patient had a stable occlusion, and the results of the orthodontic treatment were maintained. The gingival height of the maxillary left canine was stable, and this tooth showed no mobility (Fig 10).
DISCUSSION
Dental and facial esthetics of the maxillary anterior teeth should be carefully evaluated and considered when deciding which treatment option to follow. However, when the option is to keep the transposed tooth order, the orthodontist should take into account the different root prominence, the different heights of the gingival scallops, and the shape and size of the premolar.19,20 Transposition is a rare and severe positional anomaly that causes many problems during orthodontic management. The main difficulties faced when correcting the altered tooth position with maxillary premolarcanine transposition are root interference and resorption and difficulties in controlling root inclination of the transposed teeth. There are many other aspects that have to be considered such as prolonged treatment time, esthetics, function, stability, biological damage, mechanical device, and professional preference and experience. Additionally patient cooperation is an important factor that affects the treatment results. Since extraction was contraindicated after overall consideration of the cephalometric and dental cast analyses, there were 2 treatment options remaining for [Maxilla 4-3] transposition: aligning the involved teeth in their transposed positions or moving them to their correct anatomic position in the dental arch. Had the transposition not been corrected, reshaping of the incisal or occlusal surfaces should have been performed to fulfil esthetic and restorative requirements. Furthermore, for ideal function, canine guidance during lateral movement of the mandible would be needed.
Prolonged treatment time and root resorption as well as supporting tissue loss, especially of the buccal bone plate, were disadvantages of our treatment regimen. Despite these disadvantages, this treatment modality is best in terms of esthetic and functional outcomes.
We decided to align the involved teeth in their correct anatomic positions to satisfy functional, occlusal, periodontal, and esthetic demands without any reshaping procedures, including enamel reduction or restoration. Further, we used fixed biomechanics and palatal mini-implant anchorage to control tooth movement. For this patient, light forces and extra care in planning were required to avoid any possible damage to teeth and supporting structures.
To avoid root interference or resorption during treatment and to prevent bone loss at the cortical plate of the labially positioned canine, the transposed premolar was first moved palatally, enough to allow for free movement of the canine to its normal place. Then, the canine could be moved mesially to its original position in the arch.
One advantage of aligning the teeth in their correct anatomic positions with the help of palatal mini implant anchorage is that the treatment time was shortened. Therefore, root resorption as well as supporting tissue loss, especially of the buccal bone plate, were decreased and controlled in critical limits.
CONCLUSION
Orthodontic treatment of transposition is complex. Orthodontists should consider factors that could affect treatment results, such as function, occlusion, periodontal support, patient cooperation, and esthetic demands. In our case, moving transposed teeth to their correct anatomic positions in the dental arch with the help of palatal mini-implant anchorage provided excellent results in an acceptable treatment time. Post-retention records revealed the formerly transposed teeth in normal condition and the periodontal and surrounding tissues to be normal 2 years after the conclusion of treatment.








 XML Download
XML Download