

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Maintaining proper anchorage is one of the most important factors for successful orthodontic treatment. Since 1997, when Kanomi introduced titanium miniscrews, achieving maximum anchorage has became apparently easy.1 Application of mini- or microscrew implants (MSIs) may aid in achieving stable and effective intraoral, extradental anchorage without the need for patient compliance.2 MSIs offer the following advantages: small size which increases the range of possible insertion sites (alveolar process, palate, retromolar and infranasal area, symphysis, or infrazygomatic crest), easy insertion and removal, absence of complex laboratory procedures, possibility of immediate loading, and relatively low cost.1-4
Although MSIs may be used for treating many types of malocclusions and dentoalveolar discrepancies and may reduce the limitations of orthodontic treatment, MSI insertion may lead to certain complications.1,5,6 These complications include root injury, nasal and maxillary sinus perforation, nerve injury (inferior alveolar nerve, lingual nerve, etc., depending on the insertion site), MSI slippage or breakage, subcutaneous air emphysema resulting from the use of dental drills, MSI coverage by soft tissue,7 soft tissue irritation or hypertrophy, as well as inflammation causing the loosening of MSIs.3 Among these complications, root injury during MSI insertion is most commonly reported in the literature; therefore, it is of particular interest to orthodontists.3,8-10 Theoretically, the rapid evolution of precise MSI localization techniques, such as panoramic radiographs,11 dental radiographs with bisecting-angle and orthoradial-projection techniques,12 computer tomographies, 12,13 or studies conducted on prepared human jaws,14 should encourage the widespread use of MSIs by orthodontists. However, the scarcity of reports on recurrent causes of root injuries discourages the orthodontists from performing routine MSI insertions in clinical practice. Our goal therefore was to identify possible risk factors associated with root injury during implantation.
MATERIAL AND METHODS
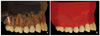
In this study, we used 35 typodonts with artificial teeth. Typodonts were made of transparent silicone material, thus enabling evaluation of possible contact between the MSI and dental root. In order to simulate clinical conditions of MSI insertion, upper parts of the typodonts were covered with opaque tape (Fig 1). Typodonts were not placed in the phantom. The orthodontist performed MSI insertion while sitting in a 9 o'clock position. Once the typodonts were established, their fixed position was supervised by the authors experienced doctors who controlled each MSI insertion process. Since the placement of the MSI into typodonts does not require apparent expansion of oral commissures, we did not simulate cheek tissues in this experiment.
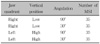
Thirty-five right-handed orthodontists underwent a 1-day theoretical training on the clinical management of MSIs. Subsequently, they inserted MSIs (AbsoAnchor®, Dentos Co. Ltd, Daegu, Korea) in the upper jaw of the typodonts, labially between the second premolar and the first molar, on the right side of the maxilla (in the low vertical position) and on the left side (in the high position). Each participant inserted 4 MSIs (core diameter of apex: 1.2 mm; total length: 8 mm) in 1 typodont using the drill-free protocol for different MSI positioning and angulations. In order to ensure an unobstructed view and to avoid bias while measuring distances between the dental roots and MSIs, the MSIs were inserted in the low position (5-mm apical from the archwire level) on the right side of the maxilla and in the high position (9-mm apical from the archwire level) in the opposite upper quadrant (Table 1). First, 2 MSIs were angulated at 90° to the alveolar process; then, they were unscrewed and inserted again, however, at an oblique angle. After each insertion, the typodonts were viewed from their bases, and this enabled evaluation of all possible contacts between the MSIs and dental roots. Because the distances between the MSI apices and artificial roots were small (in the range of millimeters), the distances were measured by placing a digital gauge on top of the model and directing the sightline perpendicularly to the top of the model.
The orthodontists were also surveyed twice, before and after the experiment, on their level of fear ranked on a 10-point visual scale. The fear levels were possibly associated with (a) risk of injury (dental root, maxillary sinus, or mandibular canal), (b) uncontrolled bur sliding while drilling, (c) breakage of either the drill or MSI, (d) bleeding, (e) bone necrosis, (f) soft tissue impaction into the drilled hole, (g) postoperative complications, (h) patient's reluctance towards MSI insertion, and (i) personal reluctance to perform surgery. The aim of the survey was to determine possible factors that would reduce fear once theoretical knowledge was supported with hands-on training. Additionally, the orthodontists listed the types of malocclusions that could preferably be managed using absolute anchorage, and this enabled evaluation of the clinical applicability and efficiency of MSI. For statistical analysis, Wilcoxon's test, chi-square test, and Mann-Whitney test were used; statistical significance was established at p < 0.05.
RESULTS
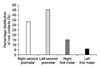
The overall root contact rate was 23.57%. Root contact (RC) occurred in 33 of the 140 insertions. MSI contact with the dental root occurred 0.94 times in the 4 trials performed by each participant; however, root contact did not occur in more than 2 trials in the case of each participant. Thirteen orthodontists did not injure any teeth; however, root contact occurred at least once in the case of trials performed by more than half the participants. The MSI predominantly contacted the premolars, and the left second premolar was injured most frequently (Fig 2).
Surprisingly, the RC rate of the MSIs inserted in the high and low positions were similar at 24.29% and 22.85%, respectively (Fig 3); furthermore, this difference was not statistically significant (p > 0.05).
MSI angulation played a significant role in the occurrence of root contact, which was more frequent when the MSI was inserted perpendicular to the long axes of the teeth (90° angulation) than when the MSI was inserted obliquely (30° angulation) (p < 0.0001); the RC rates were 45.71% and 1.43%, respectively (Fig 3). Insertion of the MSI at an angulation of 30° and in the low vertical position completely reduced the risk of root contact (Fig 4A); however, lower angulation and high position of MSI posed a risk of injury to the region neighboring the left first molar (Fig 4B).
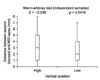
Because the number of MSIs in contact with the root of the first molar was statistically insignificant, we utilized only the distance between each MSI apex and the dental root of the premolar (DRMSI). The measured distances were classified on the basis of the low and high MSI position (Table 2) and were statistically evaluated. Mean DRMSI were significantly (p < 0.05) smaller in the right quadrant of the maxilla (low MSI position) than in the left quadrant (high MSI position) (Fig 5).
An angulation of 30° was found to increase the DRMSI 3 times in the low position and 4 times in the high position; the obtained difference was statistically significant (Fig 6). An angulation of 90° did not cause a significant difference (p > 0.05) in the DRMSI. In contrast, oblique MSI insertion in the high position significantly (p < 0.05) increased the DRMSI (Fig 6).
The fear levels of the orthodontists before and after MSI insertion were different (Fig 7). Mean fear level before the experiment was 4.6, and it significantly decreased (p < 0.05) to 3.2 after MSI insertions (Fig 8). Factors responsible for the fear levels before and after MSI insertion differed quantitatively and qualitatively (Fig 9). The fear levels before MSI insertion was mostly associated with the risk of injury to the dental root (77.14% of orthodontists), maxillary sinus (40.00%), or mandibular canal (28.57%). Only few orthodontists attributed their fear level to other factors such as uncontrolled bur sliding while drilling, breakage of either the drill or MSI, excessive bleeding, soft tissue impaction into the drilled hole, bone necrosis, postoperative complications, patient's reluctance towards MSI insertion, and personal lack of experience. After MSI insertion, the fear levels associated with the risk of injury showed an evident decrease; fear of dental root, maxillary sinus, and mandibular canal injuries were reported by 57.14%, 11.43%, and 2.85% of orthodontists, respectively. Furthermore, the spectrum of factors that affect the fear levels reduced after 4 trials; besides the risk of injury, only uncontrolled bur sliding while drilling was reported to be a factor by 2.85% of the surveyed group.
The orthodontists indicated that several types of malocclusions and dentoalveolar discrepancies could be appropriately treated with MSI support, thus proving the clinical need of absolute anchorage for dental movements in all 3 planes-vertical, sagittal, and transverse (Fig 10).
DISCUSSION
A thorough review of the literature proved that there was a lack of consensus among orthodontists regarding the reversible/irreversible biological changes after the occurrence of dental root contact. Melsen and Verna have reported that the dental pulp is not damaged in an injured tooth.3 However, this finding is not consistent with those of animal experiments. Hembree et al.15 investigated the defects caused by the intentional placement of miniscrews in the dental roots of mature beagles. They reported damages such as displacement of the alveolar bone to the periodontal ligaments, cementum, or dentin, as well as furcation defects, screw placement in the pulp chamber, and root fracture in 78.3% of teeth. Severe defects such as tissue necrosis, inflammation, and bone loss after screw placement into the furcation area were also found. Brisceno et al.16 observed either no healing or just partial healing after intentionally damaging the dental roots of beagles by using miniscrew implants when pulpal invasion and inflammatory infiltration occurred. Furthermore, Lee et al.10 established that a minimum distance of 0.6 mm between the MSI and the root was effective in preventing bone resorption and ankylosis. In contrast to the hitherto mentioned results of animal studies, the results of the study by Renjen et al. showed neither inflammation nor necrosis after intentional root injury, but continuous cementum repair was observed. When root fragmentation occurred, however, an ankylosis developed.17 Although the size of the MSI may not be a factor that causes root injury, care must be taken to minimize injuries. One possibility is the application of miniscrews with smaller diameter. According to Andreasen et al., if mechanical lesions of the periodontal ligaments are less than 4 mm2 in size, they produce transient ankylosis and subsequent healing of dental structures.18
The irreversibility of changes observed after root injury caused by MSI insertion is unclear; hence, one may conclude that root contact may not be the most important factor that affects fear levels of the orthodontists, preventing them from performing routine MSI insertion in clinical practice. Nevertheless, meticulous analysis of the literature shows that root injury is a possible and reproducible cause of premature loss of MSI; therefore, this issue warrants closer examination. Kuroda et al.12 used dental radiograms to measure the distance between the MSI and dental roots and proved that the proximity of MSI to the dental root is the most crucial factor responsible for MSI instability. Therefore, the MSI insertion in the largest interradicular region efficiently reduces MSI failure rate. Such findings were also confirmed in animal experiments conducted by Kang et al.19 who found that the MSI failure rate in beagles was much higher (79.2%) when screws were intentionally placed in the dental root than in the alveolar bone (8.3%). In light of these results, we selected the buccal site in the maxilla, which is the optimal site for MSI insertion because of the large interradicular distance. Hu et al. measured the distance between the dental roots in human maxillae after sectioning the bones and showed that the inter-root distance increased either from the anterior teeth to the posterior ones as well as from the cervical line to the apex. This distance was greatest between the second premolar and the first molar (from 6 to 8 mm above the cervical line).14 Other investigators analyzed volumetric tomographic images of 25 maxillae and established 3 buccal areas that could be used for MSI insertion at a safe distance from the dental root. These areas lie between (1) the first and second premolars, (2) the canine and the first premolar, and (3) the second premolar and the first molar and are safe for MSI insertion if the MSI is inserted above the cervical crest at 5 - 11 mm, 5 - 11 mm, and 5 - 8 mm, respectively.20 Although studies indicating the optimal site for MSI insertion have been reported in the literature, individual bone quality and thickness variations must be evaluated whenever an orthodontic treatment plan calls for maximum anchorage.13
Oblique insertion of MSI efficiently increased the DRMSI. Root contact had technically not occurred at 30° angulation of MSI irrespective of the high or low vertical position. This result is promising in terms of the clinical stability of MSIs and is in accordance with the findings of Park et al. who reported that 30 - 40° angulation of microimplant MSI in the upper jaw not only decreased the possibility of root injury but also improved MSI fixation in the bone.21 In contrast to angulation, vertical positioning of MSI did not contribute to the reduction of the risk of root injury. Overall root contact occurred at a similar rate irrespective of the high or low MSI vertical position (Fig 3).
In our study, the rate of root injury was 23.57%. Similar results have been reported by Cho et al. who investigated the rate of root contacts with MSI inserted in the anterior and lateral regions of the dental phantoms by experienced and inexperienced dentists, resulting in overall rates of root contact of 13.5% and 21.3%, respectively.8 These findings suggest that root injury incidents become less frequent as the dentists gain clinical experience; therefore, this factor must not be neglected in cases of uncomplicated MSI insertion.
We have also compared the fear levels of the orthodontists before and after MSI insertion; to the best of our knowledge, such a comparison has not been reported in the literature to date. The results of our comparison indirectly indicate the role of theoretical and practical training in encouraging orthodontists to perform MSI insertion in daily practice. In other terms, continuing education seems to play a crucial role in reducing unwanted side effects such as root contact during MSI insertion.
Our results show that root injury was not a plausible and evidence-based occurrence and hence should not prevent orthodontists from performing routine MSI insertion. In contrast to other complications such as inflammation of the peri-implant tissue that is significantly responsible for MSI loss,22,23 root contact can be controlled by adopting an angulation of 30° during MSI insertion. Elaborate surgical placement and management helps secure one of the highest success rates (93%)24 in the case of MSI insertion; this feature may also efficiently reduce the orthodontist's fear of potential root contact, as well as other factors jeopardizing MSI stability.
CONCLUSION
1. The overall rate of root contact was 23.57% (33 contacts in 140 trials). The left second premolar had the highest number of root contacts.
2. MSI angulation played a significant role in reducing root contacts. While MSI insertion in the high and low vertical positions had similar rate of root contacts, MSI insertion perpendicular to the long axes of the teeth (90° angulation) and oblique MSI insertion (30° angulation) resulted in different contact rates.
3. An angulation of 30° increased the distance from the apex of the MSI to the root of the adjacent tooth by 3 times in the low position and 4 times in the high position.
4. Providing detailed theoretical and hands-on training to orthodontists may play a role in diminishing their fear level and thus improving their learning curve.








 XML Download
XML Download