

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The skeletal Class III malocclusion can be originated from mandibular prognathism, maxillary retrognathism, or both.1,2 In most cases, Class III malocclusions are characterized by an average of a 60% maxillary deficiency.2,3 Protraction of the maxilla with a facemask is a common treatment procedure for Class III patients, with maxillary retrusion.
The use of the protraction facemask provides a directed, constant anterior force to the maxilla. With the application of constant protraction forces, several animal studies have shown significant anterior displacement of the maxillary structures, accompanied by histological changes in the circum-maxillary sutures.4,5 In addition, clinical studies indicate that the orthopedic approach is practicable for craniofacial deformities.
Studies have documented that facemask treatment before adolescence produces an orthopedic effect to place the maxilla in a forward position, often accompanied by a clockwise rotation of the mandible and counter-clockwise rotation of the maxilla, together with dental changes.6 Counter-clockwise rotation of the maxilla is beneficial in the treatment of low-angle, deep-bite Class III patients; but it has undesired effects in Class III cases with high-angle skeletal patterns and anterior open bites.6 In order to eliminate these undesired side effects, some investigators have applied the protraction force at an angle of 20 - 30° downward from the occlusal plane7,8 but others have applied the force buccally in the molar, premolar, canine, and lateral incisor regions.8-10
Hata et al.11 found that applying the force from a point 5 mm above the palatal plane (PP) resulted in elimination of the counter-clockwise rotation effect on the maxilla. Nanda12 had developed a modified protraction headgear design to deliver the protraction forces from a higher level. Alcan et al.13 introduced the modified maxillary protraction facemask where they applied the point of force up to the level of the forehead. Keles et al.6 examined the effect of varying force directions on maxillary protraction by modified facemask appliance and found that this method can be used effectively on patients who represent Class III malocclusion combined with anterior open bite. Göyenç and Ersoy14 evaluated the effects of modified facemask therapy on dentofacial structures. They concluded that, applying the force with modified facemask by means of a facebow induced anterior movement of the maxilla without rotation of the jaws and upper and lower maxillary heights were unaffected.
To our knowledge there is no research in the literature that compared the effects of conventional and modified facemask appliances; and evaluated with a control group all in one study. The purpose of this prospective study was to evaluate the dentofacial effects of conventional and modified facemask therapies with rapid maxillary expansion, in Class III patients; and compared with an untreated control. For group 1, the protraction force was applied intraorally from the lateral region, in group 2 the protraction force was applied with a modified facebow extraorally from a higher level and group 3 consisted of control subjects.
MATERIAL AND METHODS
This study was approved by the Regional Ethical Committee on Research of the Erciyes University, Faculty of Dentistry.
A power analysis established by G*Power Ver. 3.0.10. (Franz Faul, Universität Kiel, Germany) software, based on a 1:1 ratio between groups, showed the a sample size of 21 patients would give more than 80% power to detect significant differences with 0.40 effect size and at α=0.05 significance level.
The samples consisted of cephalometric records of 72 Class III patients with maxillary retrusion. Patients who fulfilled the following inclusion criteria were selected:
Class III molar relationship
Anterior crossbite or edge-to-edge incisal relationship
ANB angle of 0° or less; and nasion perpendicular to A-point of 2 mm or less
No congenitally missing or extracted teeth
No deformity in the nasomaxillary complex
Cephalometric radiographs of adequate quality available before and at the end of facemask-expansion therapy.
Patients with craniofacial abnormality, psychosocial impairment, craniofacial anomaly or skeletal openbite (at least a 1 mm opening when the incisal edges of the maxillary and mandibular incisors were projected perpendicularly onto the N-Me plane) were excluded from the study.
Sixty-nine (36 girls and 33 boys) out of the 72 subjects who met the inclusionary criteria were randomly selected, and 3 patients were discarded because of psychosocial impairment, craniofacial anomaly and insufficient cooperation. Conventional facemask treatment group (Group 1) comprised of 24 patients, 13 girls and 11 boys (mean age, 9.2 ± 1.4 years); modified facemask treatment group (Group 2) comprised of 24 patients, 12 girls and 12 boys (mean age, 9.3 ± 1.6 years); and control group (Group 3) comprised of 21 subjects, 11 girls and 10 boys (mean age, 9.8 ± 1.9 years).
Cephalometric records were obtained from all subjects at pre- and post-treatment for the experimental group, and during the control period for the control group. Treatment time in Group 1 ranged between 0.5 and 1.7 years (mean 1.09 ± 0.28 years); treatment time in Group 2 ranged between 0.7 and 1.8 years (mean 1.2 ± 0.3 years); and the observation period ranged between 0.5 and 1.7 years (mean 0.91 ± 0.36 years).
To constitute the control group, cephalometric records were taken with parental permissions by obtaining informed consent from subjects/parents; who did not accept treatment by an extraoral appliance, at that time. Then most of these subjects accepted the treatment protocol.
Appliance design in group 1
In this group, a facemask,15 and a bonded full coverage maxillary acrylic splint expander with vestibular hooks, and heavy elastics (500 g, depends on the distance between the hooks of expansion appliance and the facemask) were used for orthopedic facemask therapy.8
Elastics were connected bilaterally to an adjustable midline crossbow on the Petit type facemask.15 The protraction elastics were applied to the vestibular hooks attached between the lateral incisor and canine teeth 10 - 15 mm above the maxillary occlusal plane (Fig 1); with a downward and forward pull of 20° to avoid bite opening during maxillary protraction (Fig 2).
Appliance design in group 2
A modified bonded rapid maxillary expansion appliance with full occlusal coverage, a specially designed facebow, a facemask and heavy elastics (500 g, depends on the distance between the modified facebow hook parts and the facemask) were used for orthopedic facemask therapy.
The bonded expansion appliance was modified by adding two tubes (Activator Tubes, Dentaurum, Ispringen, Germany) on the buccal side of the acrylic in the premolar area (Fig 3). The purpose of these tubes was to accommodate the inner bows of the specially designed face bow. The facebow was constructed from an adjustable facebow (Std Ss Facebow, G&H Wire Company, Franklin, Indiana, USA). The inner bows of the facebow end in the mouth with a special U-shaped bend in order to enter the buccal tubes from the distal, and thus be able to retain it, when an anterior pull is applied. The outer bow was bent upwards at a 90 degree angle to provide a point of force application at the level of the dentomaxillary center of resistance, and also to apply the parallel forces on both sides (Fig 4).
In both treatment groups, the midline expansion screw of the bonded maxillary expander was activated two times a day for the first week and once a day until the desired change in the transverse dimension was achieved. Patients were instructed to wear the facemask full-time except during meals. We told patients to keep track of his/her wearing time on the scorecard and to bring his/her card to each visit. The appliance was used in both treatment groups until a positive overjet was accomplished.
Cephalometric analysis
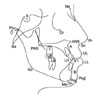
All of the cephalometric films used in this study were taken in the same cephalostat (Planmeca; Planmeca OY, Helsinki, Finland). All subjects were positioned in the cephalostat with the sagittal plane at a right angle to the path of the X-ray, the Frankfort plane was parallel to the horizontal, the teeth were in centric occlusion, and the lips were lightly closed.16 All hard and soft tissue landmarks were digitized and measured with Dolphin Image Software, Version 11.0 (Dolphin Imaging and Management Solutions, Los Angeles, California, USA). Twenty measurements, (9 linear and 11 angular) were used to evaluate the changes in treatment and control groups. The landmarks were identified according to the definitions provided by Swlerenga et al.17 and presented in Table 1. Landmarks used in this study are shown in Fig 5.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences, version 13.0 for Windows (SPSS Inc., Chicago, IL, USA). Arithmetic mean and standard deviation values were calculated for all cephalometric measurements. The normality test of Shapiro-Wilks and Levene's variance homogeneity test were applied to the data. The data were found not normally distributed, and there was no homogeneity of variance between the groups. Intra- group comparisons were evaluated by using non-parametric Wilcoxon's test and intergroup changes were analyzed with Kruskal-Wallis test. The statistical significance of intergroup differences was further assessed with the Mann-Whitney test for independent samples with Bonferroni's correction (p < 0.016).
To determine the errors associated with radiographic measurements, 10 radiographs were selected randomly. Their tracings were repeated 8 weeks after the first measurement. A Bland and Altman plot was applied to assess the repeatability. It was found that the difference between the first and second measurements were insignificant (Table 2).
RESULTS
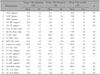
Pre-treatment/control values and standard deviations of measurements and statistical comparisons are presented in Table 3. Pre- and post-treatment/control descriptive statistical values and comparisons are presented in Table 4.
Pre- and post-treatment and pre- and post-control intra-group comparisons
In group 1, post-treatment measurements showed statistical changes in Pog to N perp (p < 0.05); SN-MP (p < 0.01); and SNA, ANB, A to N perp, N-Me, ANS-Me, and Upper lip to E plane (p < 0.001).
In group 2, post-treatment measurements showed significant differences in U1-NA (mm), U1-NA (°) and L1-MP (°) (p < 0.05); A to N perp and Upper lip to E plane (p < 0.01); and SNA, SNB, ANB, SN-MP, Pog to N perp, N-Me, ANS-Me, interincisal angle, L1-NB (mm), L1-NB (°), and Lower lip to E plane (p < 0.001).
In group 3, post-control measurements showed increases in SNA, N-Me, N-ANS, U1-PP (p < 0.05) and SNB measurements (p < 0.01).
Treatment and control changes between group comparisons
In group 1, SNB changes were less than the control and this changes were statistically significant (p < 0.05). There were increases in SNA, ANB, SN-MP, (p < 0.001) and A to N perp and Upper lip to E plane (p < 0.01).
In group 2, SNB, U1-NA (°) (p < 0.05) and U1-NA (mm) and Pog to N perp (mm) (p < 0.01) changes were less than the control. There were increases in SNA, SN-MP (p < 0.01) and ANB, A to N perp and Upper lip to E plane (p < 0.001).
When both treatment groups were compared, no statistically significant differences were found in any of the measurements.
DISCUSSION
To our knowledge, the present study is the first to evaluate and demonstrate the effects of a modified facemask (protraction force applied with a modified facebow extraorally); and to compare it with the conventional facemask and an untreated control group, all in one study. In this study, both treatment groups showed that the SN-PP angle did not change and the maxilla showed no rotation while moving forward.
The average age of patients that were selected for the study group was 9.43 years. A review of the literature reveals that greater skeletal changes with the use of the maxillary protraction appliance are possible in young patients.18,19 Treatment in the deciduous dentition produces greater skeletal changes than those produced in the mixed dentition stage;20 moreover, when therapy begins in the early mixed dentition, it seems to induce more favorable changes in the craniofacial skeleton, compared with the same treatment started in the late mixed dentition.21 However, Baik22 reported that comparison of the measurements of the treatment effect according to age showed no statistically significant difference. Similarly, Yüksel et al.23 compared the treatment outcomes in two different chronological age groups and found no significant difference in the orthodontic and orthopedic effects. According to, Merwin et al.24 there was no difference between the age groups 5 to 8 and 8 to 12 years from the point of protraction of the maxilla.
Proffit and Fields25 claimed that rapid maxillary expansion (RME) had to be carried out, before protraction of the maxilla. There are other studies12,26 in the literature that support the concept that, RME treatment releases maxilla's sutures with the surrounding bones and enhances the protraction procedure. In the present concept, treatment was started in the seventh day of RME in both treatment groups after mobilizing the sutures surrounding the maxilla.
During the protraction procedure, rigid appliances are needed to withstand the heavy forces.13 For this purpose some investigators have used rigid wires,27 whereas others used an acrylic cap splint.26 Previous investigations8 showed that the application of cap splint type maxillary expansion appliances would increase the skeletal effect of the protraction headgear. In the current study, a full coverage maxillary acrylic splint expander appliance was used in both treatment groups, in order to increase the rigidity of the appliance, to prevent the occlusal interferences, to apply homogeneous force, and to maximize the skeletal effect of the protraction headgear.
Class III malocclusions could have beneficial effects from early orthopedic intervention, but cases should be selected carefully. The facial growth pattern, age, heredity and amount of pretreatment overbite and overjet are factors to be considered for prognosis and also for prevention of relapse.28 For that reason, patients presenting normally directed vertical growth patterns with normal overbite were included but patients with craniofacial anomaly, psychosocial impairment, or skeletal openbite were excluded from the study.
Conventional and modified facemasks have different biomechanical properties. In the conventional facemask group, force was applied below from the center of resistance of the maxillary dentition. On the other hand, in the modified facemask group, force was applied from the maxillary incisor root apex area. As a consequence, the maxillary incisor teeth were retroclined.
Both treatment groups demonstrated significant responses to facemask/expansion therapies, which affect many areas of the dentofacial complex, when compared to the control group. Skeletal change was primarily a result of an anterior movement of the maxilla. When the treatment groups' maxillary change was compared to the control, the results confirmed a maxillary orthopedic effect resulting from treatment (change in SNA: Group 1, 3.9°; Group 2, 3.8°; Group 3, 0.7°; change in A to N perp: Group 1, 3.2 mm; Group 2, 2.9 mm; Group 3, -0.50 mm). Ishii et al.10 and Mermigos et al.7 have reported similar findings for maxillary movement.
Many investigators have stated that facemasks worsened the vertical growth pattern in Class III cases characterized by maxillary retrognathism and an openbite tendency.24 The reason for this was the counter-clockwise rotation of the maxilla that occurred in patients treated with facemask therapy.6 Frequently counter-clockwise rotation of the maxilla brought aggravation in the vertical dimension. Authors10,18 observed significant rotation of the palatal plane with conventional facemask appliance. Palatal plane rotation was not observed in the present study for both treatment groups. The rotation of the palatal plane described in other studies may be affected by many factors, including site of force application, direction of elastic traction, as well as the facial pattern of the patient. Hata et al.11 studied the effects of changing the level of force application on the maxilla during protraction procedures. Studies were carried out on dried skulls and facemasks were used while applying the force from different levels. The researchers found that applying the force from 10 mm above the palatal plane resulted in elimination of the counter-clockwise rotation effect on the maxilla.11 All patients in Group 1 were treated with elastic traction attached in the area of the lateral incisor hook which is 10 - 15 mm above the maxillary occlusal plane, with the direction of pull predominately downward (20°) from the horizontal. In group 1, as a consequence of this procedure, the maxilla moved anteriorly without rotation. In group 2, patients were treated with the modified facemask and this allowed the point of force application to be provided at the level of the dentomaxillary center of resistance. Keles et al.6 and Göyenç and Ersoy14 investigated similarly designed modified facebow effects and they stated that anterior translation of the maxilla without rotation had occurred. The results for group 2 from the present study were similar to these research.
Clockwise rotation of the mandible is ideally suited for patients with excessive overbite and vertical maxillary deficiency. It should be noted, however, that the subjects in this study did not demonstrate severe vertical growth patterns and an openbite tendency. Significant changes in the mandibular position also contributed to the Class III correction. Downward and backward movement of the mandible that was shown in both treatment groups was consistent with other investigators.10,18 In contrast, Mermigos7 who used maxillary protraction alone, reported that the mandibular plane remained unchanged. Mandibular rotation may be due to a combination of vertical maxillary movement, eruption of the maxillary molar, and a distalizing or retraction force on the chin.19 Baccetti et al.21 observed a backward positional rotation of the mandible associated with an increase in lower anterior facial height in Class III patients treated with the facemask. Consequently, a redirection of future mandibular growth in a more downward and backward vector could be expected after treatment due to extrusion of maxillary posterior teeth and downward growth of the maxilla.
Dental changes related to orthopedic protraction forces to the maxilla have been widely studied and maxillary incisor protrusion have been reported.18 These researchers found maxillary counter-clockwise rotation; however, this rotation may reflect the maxillary incisor position. In group 1, the maxillary incisor position did not change with the treatment. However, in group 2, U1-NA measurements were increased, but U1-PP measurement was stable because of maxillary parallel anterior movement.
Macdonald et al.29 stated mandibular incisors become upright after treatment whereas Ngan et al.30 and Baik22 reported a decrease in the inclination of the lower incisors. In both treatment groups, lower incisor inclination could not be changed with facemask therapy. Because facemasks have different biomechanical properties, lower incisor inclination was decreased in group 1 and was increased in group 2 but these changes were not statistically significant. Similarly Göyenç and Ersoy14 used the modified protraction headgear and they did not report any changes in lower incisor position.
Significant correlations were found between changes in the sagittal relationships of the skeletal and soft tissue profiles in both the maxilla and mandible.1 Kapust et al.19 reported forward movement of the upper lip and retraction of the lower lip. In this study we determined that the upper lip moved forward; but lower lip position did not change during the therapy for both treatment groups.
Future studies are needed in order to examine the long-term stability of the skeletal and dental changes related to the maxilla and mandible.
CONCLUSION
Modified facemask appliance can be used effectively in Class III patients with a retrognathic maxilla. Facemask therapies with expansion resulted in an anterior advancement and translation of the maxilla without rotation and the mandible moved downward and backward in both treatment groups. Both treatment protocols have similar effects except for incisor positions.






 XML Download
XML Download