

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Skeletal Class III malocclusion is a common malocclusion in orthodontic clinics in China.1 It often presents the clinician with extreme difficulties for successful treatment. Studies have reported that skeletal Class III discrepancy worsens with age.2,3 Early intervention of skeletal Class III deformities in the mixed dentition or even in the deciduous dentition has received increasing attention in the orthodontic field. The alternative approaches include the use of reverse headgears, chin cups and functional appliances.4-8 However, not all patients can achieve good results using these methods. Furthermore, the patient seeking treatment at the clinic may be past their adolescent growth spurt and present with a severe skeletal Class III deformity. In some of these patients, treatment with either surgical-orthodontic therapy or orthodontic camouflage treatment is possible. We refer to these cases as the "borderline case". For adult borderline skeletal Class III patients, orthognathic surgery is often the recommended choice of therapy as this can achieve a good result and the outcomes tend to be stable. However, in China, some patients do not readily accept surgery because of economical and psychological reasons as well as the potential surgical risks involved. Can orthodontic camouflage treatment achieve a similar result as successful as orthognathic surgery?
Lin and Gu9 reported that they had successfully treated 13 severe skeletal Class III cases using the method of extraction of two lower second molars. After treatment, the soft tissue change was remarkable and concave facial profiles were improved to straight profiles. Sato10 introduced the MEAW (multiloop edgewise archwire) therapy with extraction of two lower third molars for skeletal Class III patients. In our clinic, we conducted a search for the available treatment methods for adult borderline skeletal Class III cases using orthodontic camouflage treatment. For example, extraction of two lower first or second premolars was used to treat skeletal Class III malocclusion and a Class III molar relationship and proper overjet and overbite were achieved at the end of the treatment.
The aim of this study was to evaluate dentoskeletal and soft tissue profile changes after extraction of two lower first or second premolars in adult borderline skeletal Class III cases.
MATERIAL AND METHODS
Cases selection
Fifteen males and thirteen female consecutive patients with "borderline" skeletal Class III malocclusion were included in this study. The ages of the patients ranged from 17.0 to 22.4 years with a mean age of 18.8 years. All the patients were treated with extraction of two lower first or second premolars in the Department of Orthodontics at the Fourth Military Medical University. The patients' first visit dates were all from 2002 to 2007. The study protocol was approved by the Ethics Committee of the Fourth Military Medical University and informed consent was obtained from patients. The selection criteria were as follows:
(1) Anterior crossbite;
(2) Mesial or superior mesial Class III molar relationship, with maxillary second premolar occluding in the buccal groove of the mandibular first molar;
(3) No mandibular shift due to occlusal interference or premature contact of teeth;
(4) Concave facial profile;
(5) -4.0° ≤ ANB < 0°;
(6) Over the adolescent growth spurt;
(7) Originally classified as surgical cases by other orthodontists but the patients and their families rejected surgical treatment.
Treatment approach
All patients were treated with the standard edgewise technique. In these cases, two lower first or second premolars were extracted. The basis for making extraction decisions of first vs. second premolars was as follows: Commonly, the two first premolars were extracted to correct the marginal Class III cases. However, if the second premolars were carious, then the decayed teeth were extracted. Also, the reversed overjet and molar relationship should be considered when extraction. If the reversed overjet distance was short and the molar relationship was not a superior mesial Class III, then the second premolars were considered to be extracted to correct the molar relationship. Class III elastics were used in some cases when required. Light and continuous force was recommended (about 50 g on each side) and the "torque" force in the lower anterior teeth was used to avoid the lingual inclination. TAD were not used for anchorage control in this study. The mean duration of treatment was 2.0 ± 0.6 years.
Cephalometric analysis
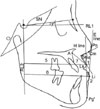
Standardized lateral cephalometric radiographs of each patient were obtained at the start and end of treatment. Each radiograph used in the present study were taken in the same cephalostat and traced on acetate paper. Twenty-five cephalometric landmarks (Figs 1, 2, 3) were identified.11-14 All the tracings and measurements were manually carried out twice with a 2-week interval by one examiner with a sharp pencil under optimal conditions.
Statistical analysis
The statistical analysis was processed with SPSS 10.0 for Windows. The arithmetic mean and standard deviation were calculated for each variable. Paired t-tests were performed to assess the statistical significance of any dental and skeletal change. The levels of significance were: p ≥ 0.05 (NS), *p < 0.05; †p < 0.01.
The method error in locating, superimposing and measuring the changes of different landmarks was calculated by Dahlberg's formula  , where d represents the difference between two registrations and n is the number of duplicate registrations. The method error determined was 0.3 mm for linear measurement and 0.4° for angular measurement, which were both statistically insignificant (p ≥ 0.05).
, where d represents the difference between two registrations and n is the number of duplicate registrations. The method error determined was 0.3 mm for linear measurement and 0.4° for angular measurement, which were both statistically insignificant (p ≥ 0.05).
, where d represents the difference between two registrations and n is the number of duplicate registrations. The method error determined was 0.3 mm for linear measurement and 0.4° for angular measurement, which were both statistically insignificant (p ≥ 0.05).RESULTS
After using the standard edgewise technique and extraction of two lower first or second premolars, most of the patients achieved efficient treatment. At the end of the treatment, the facial profile was improved from a concave to a straight tendency. The anterior crossbite was corrected and a Class III molar relationship and Class I canine relationship were achieved in all subjects. There was no sign of active periodontal disease or gingival inflammation after treatment. The occlusal relationship in the upper and lower arches was stable, tight and concordant after the treatment.
Skeletal and vertical changes
No significant anteroposterior or vertical skeletal changes were identified during treatment (p ≥ 0.05). The ANB angle increased by 0.4° and the mandibular plane angle increased by 0.6° but were significantly different (p ≥ 0.05). The occlusal plane angle (OP-FH) rotated counterclockwise with a mean value of 0.9° (p ≥ 0.05).
Dental changes
The upper incisors to the SN plane were proclined a mean of 3.6° (p < 0.05). L1-MP angle decreased by 8.1°, U1-L1 angle increased by 7.7°, L1-NB angle decreased by 7.3° and L1-NB distance decreased by 4.8 mm (p < 0.01). The overjet was increased by 5.7 mm (p < 0.01) (Table 1).
Soft tissue changes
After treatment, the results were statistically significant with Cm-Sn-Ls decreased by 3.1° and Ls-E distance increased by 0.9 mm (p < 0.05). Also Li-E distance decreased by 3.2 mm, Li-H distance decreased by 3.4 mm and Li-RL2 distance decreased by 4.1 mm (p < 0.01) (Table 1).
Case report
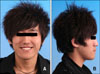
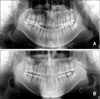
A 17-year-old male presented with anterior crossbite and mandibular protrusion (Figs 4, 5, 6, 7, 8, 9, 10). The intraoral examination showed a Class III molar relationship on both sides and slight crowding in the upper and lower arches. A crossbite from 14 to 22 was noted. The overjet was -2 mm and ANB angle was -4°. The mandibular dental midline was 2 mm to the left of the facial midline. Therefore, a combined surgical-orthodontic treatment was recommended, but the patient refused this treatment. Treatment started with extraction of two lower first premolars and standard edgewise technique was applied. In order to avoid the occlusal interference during buccal movement of upper teeth, a lower bite-plate was fitted. The bite-plate was then transferred to the upper arch after extraction of two lower first premolars. After eight months of retraction of the mandiblular anterior teeth and Class III elastics, the anterior crossbite was corrected. Sixteen months later, a Class III molar relationship and Class I canine relationship was established with a corrected midline. At the end of treatment, the concave facial profile of the patient was changed to a straight profile. The overjet and overbite were normal without deleterious effects to the periodontium and the lower incisors were stable. The active treatment time for this patient was twenty three months. The skeletal Class III tendency remained after treatment with an ANB angle of -3.5°, but the facial profile showed significant improvement.
DISCUSSION
Select identifications for treatment in "borderline skeletal Class III malocclusion"
"Borderline" surgical/orthodontic cases refer to patients with mild to moderate skeletal problems that can be treated by either orthodontic or surgical means.15 Cassidy et al.16 defined "borderline cases" as those patients who were similar with respect to the characteristics on which the orthodontic/surgical decision appeared to have been based. As for the adult skeletal Class III cases, however, how should clinicians determine if patients are suitable for surgery? It still lacks a clear consensus.9,17,18 Kerr et al.17 tried to establish some cephalometric yardsticks in adult patients with class III malocclusion to find objective criteria for treatment options. These researchers indicated that surgery should be performed for patients with an ANB angle of less than -4°, a maxillary/mandibular (M/M) ratio of 0.84, an inclination of the lower incisors to the mandibular of 83°, and a Holdaway angle of 3.5°. In 2002, a formula was developed to determine whether patients with class III malocclusion underwent either orthodontic treatment or orthognathic surgery, on the basis of the four variables: Wits appraisal, length of the anterior cranial base, M/M ratio, and lower gonial angle.19 Zeng et al.18 reported that orthodontic doctors should consider orthognathic surgery when the ANB angle was under -4° and L1-MP angle was under 82°. Ning et al.14 suggested that orthodontic camouflage treatment could achieve good results when the ANB angle was from -3° to 0°. However, these studies did not provide methods to specifically distinguish between patients with "borderline" surgical-orthodontic class III malocclusion. Furthermore, the treatment choices largely depended on the clinicians' personal preferences. In our research for all patients, the ANB angle was under 0° and the lowest value was -4.0°. Using the orthodontic camouflage treatment, all patients achieved a proper overjet and overbite.
Influence of extraction of two lower first or second premolars on skeletal, dental and soft-tissue profiles
Extraction of two lower first or second premolars has little effect on skeletal parameters and there were no statistical significance observed (p ≥ 0.05). The change in ANB angle was not obvious with a value of -2.0° after treatment. This proved that orthodontic treatment of skeletal Class III cases with the extraction method had camouflage effects and surgical-orthodontic treatment should be suggested for severe skeletal Class III cases to achieve a good effect. In our study the change seen in the lower incisors was significant with several items changing significantly (p < 0.01) due to the extraction of premolars in the mandible. After treatment, the overjet and overbite was proper. Pellegrino G20 and Fukui and Tsuruta et al.21 both reported a skeletal crossbite case with severe crowding in the upper and lower arches. Both of the patients were treated by extraction of four premolars. The overjet and overbite became normal after treatment and good occlusal relationship was achieved with straight profiles attained. Our results with cephalometric radiographs were consistent with their study. When closing the extraction space in the mandible, we should pay close attention to the thickness of the buccal plate and avoid excessive lingual inclination during retraction. The improvement in soft tissue profile was obvious with concave profiles before treatment changing to straight profiles after treatment. The imbalance of soft tissue change and skeletal change after orthodontic treatment is valuable as a nonsurgical treatment of severe skeletal Class III malocclusion.1,9 Also, the compensatory mechanism is worthy of further study.
The tongue position of Class III patients is quite large and flat. The forceful tongue could cause relapse, and also occlusal trauma to upper anterior teeth could occur if the lower teeth are uprighted due to force from the tongue. For this, we instruct the patients to do tongue exercises and ask them to wear retainers carefully for at least two years.
Comparison of the extraction of two lower first or second premolars with other extraction modes for camouflage treatment of skeletal Class III malocclusion
According to the study by Lin and Gu,9 the indications to extract two lower second molars include severe skeletal Class III malocclusion, a mesial relationship of first molars and a well arranged arch or only minor crowding of the lower arch. Compared with extraction of two lower second molars, whether the third molar erupted into the second molar's place was not a concern when using our method. Also, after the extraction of two lower second molars, all of the teeth including the first molars in the mandible need to be retracted back one at a time. The distance moved is relatively long and the number of teeth moved is more than that required during extraction of the two lower first or second premolars. In our study, the extraction space was closed by moving the anterior teeth backwards and posterior teeth forwards. The distance moved and the treatment time were relatively short. In the study by Lin JX, the mean treatment time was comparatively longer, about 2.6 ± 0.6 years, but in our study the mean treatment time was 2.0 ± 0.6 years.
Another extraction method in the treatment of skeletal Class III malocclusions was extraction of one lower incisor. This method was adopted for mild Class III malocclusions and was noted for a shorter treatment time. However, a midline deviation existed and stable interlocking occlusal relationship was not easily achieved after treatment.
For camouflage treatment in skeletal Class III cases combined with severe crowding, the extraction of four premolars in the upper and lower arches was adopted at times. Ning et al.14 indicated that the upper arch length discrepancy should be carefully analyzed before extraction of two upper premolars. Otherwise the facial profile may be poor due to over-retraction of the anterior teeth. The mean treatment time was 2.1 ± 0.4 years.
In orthodontic treatment, we have objectives to be met which are function, esthetics and stability. However, because long-term records are not yet available for this treatment group, caution is advised in assuming the permanency of acceptable outcomes at this time. Proper diagnosis and the establishment of realistic treatment objectives by the clinician and the patient are necessary to prevent undesirable sequelae in Class III camouflage treatment.
CONCLUSION
Extraction of two lower first or second premolars provides a viable treatment alternative for skeletal Class III cases to achieve good results.
After treatment, the overjet and overbite were normal and Class III molar relationship and Class I canine relationship were achieved in all subjects. The occlusion relationship was stable, tight and concordant.








 XML Download
XML Download