

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
One of the most important objectives of orthodontic treatment is to achieve a stable occlusion, with the periodontal ligaments typically returning to their pretreatment dimension after removal of orthodontic forces.1 A limited amount of post-treatment change is acceptable and often desirable to permit settling of the occlusion. Most orthodontic treatment results, however, potentially are unstable, and therefore retention is necessary to prevent relapse following fixed appliance removal.
One method to evaluate the periodontal stabilization following orthodontic treatment is to assess tooth mobility, which decreases progressively after removal of an orthodontic force. Miller2 has proposed a classification of tooth mobility and has categorized greater than normal mobility as scores of 1, 2 and 3. Quantifying such movements objectively and precisely has been a challenge clinically, however, which has led to the development of numerous measuring instruments.3-6 The use of the Periotest®, a non-invasive, electronic device that provides an objective measurement of the reaction of the periodontium to a defined impact load, has been reported to be a highly accurate, objective and reproducible method of evaluating tooth mobility.7,8
Nakago et al.9 investigated the relative mobility of four canines after orthodontic tooth movement using the Periotest® methodology. A major purpose of their study, however, was to assess the efficiency and reliability of these instruments for clinical use. Tanaka et al.10 investigated the alteration of tooth mobility through orthodontic treatment using the Periotest® in 83 individuals. They measured the mobility before and after orthodontic treatment and after retention, and suggested that the tooth mobility may be one of the useful indicators for determination of the duration of the retention period.
The purpose of the present study was to evaluate the changes in tooth mobility using the Periotest® protocol following orthodontic tooth movement and to obtain information regarding the timing and required duration of periodontal stabilization during the retention period.
MATERIAL AND METHODS
Sample
Twenty orthodontic patients who had been treated with edgewise appliances were used as subjects in this study. They were selected regardless of age, sex, or treatment modality (e.g., extraction or non-extraction). Fifteen patients were treated non-extraction, and five patients had extractions as part of their treatment regimen. Following active treatment, a removable type of retainer, Begg type, was used in the maxillary arch, while either a removable retainer or a canine-to-canine bonded lingual retainer was used in the mandibular arch. The removable retainers were worn on a full-time basis for the first six months and subsequently for as many hours as possible, including nighttime.
Methods
The mobility of the maxillary teeth from the central incisor to the first molar was measured bilaterally with the Periotest® instrument (Siemens AG, Bensheim, Germany) at three-month intervals. In other words, tooth mobility was measured at the time of the removal of the orthodontic appliance, and at 3, 6, 9, 12, 15, 18, 21, and 24 months following appliance removal.
To perform the measurement using the Periotest® device, an investigator held a handpiece close to the facial surface of the tooth and started the measurement. During the procedure, the handpiece was held perpendicular to the long axis of the tooth, and the point of impact was the middle of the anatomical crown (Fig 1).
It has been shown that when the Periotest® device is used improperly, it underestimates the degree of tooth mobility.11 Thus, to reduce the measurement error, tooth mobility was measured three times, and the maximum value was selected. Mean and standard deviation of Periotest® values (PTV) were calculated for each tooth, and the total PTV was computed. A repeated measures ANOVA was performed to determine the statistical significance of the differences between time intervals, and the contrast method12 was used for pairwise comparisons. Each measurement was compared with the previous measurement as the contrast. A significance level of α= 0.05 was selected.
RESULTS
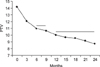
Table 1 shows the means and standard deviations of tooth mobility and the changes in the Periotest® value for each tooth at each observation period. A common feature among all teeth was a gradual decrease in tooth mobility over time. The comparison of mobility at three-month intervals is shown in Fig 2, which indicates that tooth mobility decreased rapidly during the first six months, decreased more slowly during the next six months, then tended to plateau during the final twelve months of the study. The decreases were statistically significant during the first year except for the period between six and nine months. The changes, however, were not statistically significant during the second year following appliance removal.
DISCUSSION
One of the most important objectives of orthodontic therapy is the maintenance of the treatment outcomes over the long-term. It is well known that teeth often exhibit a tendency to move back toward their original position after removal of the orthodontic appliances. This relapse is due in part to the contraction of the stretched fibers of the periodontal ligament.1 If the teeth are not retained sufficiently, relapse may occur. Thus, a regimen of retention is necessary after orthodontic treatment in order to allow for adequate remodeling of the stretched periodontal fibers.
Many studies have been conducted in an attempt to determine the optimal duration of periodontal stabilization.13-15 An histological approach cannot be applied to patients directly, and a radiological approach can be considered strongly subjective in nature; neither is helpful in assessing the stabilization of the periodontal ligament. Tooth mobility, however, can be used on a longitudinal basis as an indicator of biological changes within the periodontal ligament. Tooth mobility increases during orthodontic treatment as a result of the widening of the periodontal ligament space and then gradually decreases to physiologic mobility after the removal of the appliance.1,16
Miller2 has described three stages of excess tooth mobility. A score of 1 indicates the first distinguishable sign of movement greater than normal. A score of 2 indicates a movement that allows the crown to move 1 mm, and a tooth with a mobility score of 3 moves more than 1 mm. Such a classification system, while useful clinically, is non-scientific, highly subjective to individual interpretation, and may be inaccurate.
Many approaches have been devised to measure tooth mobility more precisely. Mühlemann4,5,17 used two different intraorally-attached dial indicators to study the degree of mobility; Goldberg18 used a modified periodontometer to measure tooth mobility during various types of periodontal therapy. In addition, O'Leary and Rudd19 designed an instrument similar to the macroperiodontometer to investigate the range of tooth mobility in healthy mouths, and Burstone et al.6 applied holography to the study of tooth displacement. Their instruments and procedures, however, were either inconvenient or impractical to apply to patients on a routine basis.
The Periotest® instrument was designed to provide an objective measure of tooth mobility, with a decrease in Periotest® values indicates increased resistance to tooth mobility. An increase in values shows decreased resistance, and thus indicates the potential for tooth mobility. The Periotest® is known as an instrument that is highly accurate and reproducible: a simple and easy-to-manage objective methodology.7,8
During measurement, the Periotest® handpiece always must be held perpendicular to the long axis of the tooth, and the point of impact must be the middle of the anatomical crown. As mentioned earlier, the device is suspected to underestimate the degree of tooth mobility in instances of improper use.11 Thus, tooth mobility was measured three times, and the maximum value was recorded.
It should be noted that the rest position of a tooth in the alveolar socket is not constant. Teeth are intruded slightly by occlusal forces during mastication and extruded if occlusal contact is avoided for one to three hours. Moreover, mobility values may fluctuate during the day.5,20 With these factors in mind, tooth mobility for ten selected control subjects was measured three times, with a 24 hour-interval between recordings, and then values were analyzed according to Dahlberg's formula.21 As a result, the method error was low (PTV = 1.1).11
Van Scotter and Wilson22 compared the mobility index of Miller2 to the Periotest® values. Normal tooth mobility ranges from PTV -8 to 9, Mobility #1 from PTV 10 to 19, Mobility #2 from PTV 20 to 29 and Mobility #3 from PTV 30 to 50. Accordingly, the method error of the PTV in the study (i.e., 1.1) was acceptable to measure the tooth mobility.
Only maxillary teeth were selected as samples in this study. Schulte and his associates8 investigated the Periotest® values of the maxilla and mandible dentitions. Periodontally healthy teeth had higher Periotest® values in the maxilla, which has more cancellous bone than the mandible. In that maxillary teeth show a higher amount of mobility, they can be considered to be more acceptable to serve as samples to evaluate the degree of periodontal stabilization over time.
There also was a practical reason for selecting only the maxillary teeth; a bonded type of retainer was used in the mandibular arch for some individuals. In the current study, the use of only maxillary teeth as samples was felt to be sufficient, in that the main objective of the study was to investigate the change in mobility according to time elapsed after appliance removal.
In comparing variations in mobility among teeth, Periotest® values of the incisors and premolars scored higher than did those of molars and canines at each visit. This finding indicated that tooth mobility may be related to total root surface area. Teeth with larger root surface areas had a greater surface area for the attachment of periodontal fibers, which apparently made them more stable than teeth with small root surface areas.7,8,23
Jepsen23 measured the root surface area of the maxillary and mandibular teeth previously. Total root surface area was the greatest in the first molar, followed by the canines, premolars, and incisors. The order reported by Jepsen23 was identical with that of Tylman and Tylman24 and Watt et al.25 In the instance of canines, however, the total root surface area did not explain these findings adequately. Surprisingly, the canines showed Periotest® values lower than those of the first molars, indicating greater relative stability. The reason may be that canines have the longest root in the arch, and the leverage effect resulting from its crown-to-root ratio was responsible for the lower Periotest values.8,23
In evaluating tooth mobility at three-month intervals during the two years following appliance removal, there was a rapidly decreasing pattern of mobility for the initial six months, a slow decrease after six months, and no significant decrease after twelve months. It is well known that the gingival fibers are disturbed by orthodontic tooth movement and must remodel to accommodate the new tooth positions. In a study investigating the biomechanical behavior of the canine periodontium of 10 adolescent patients, Tanne et al.16 reported that the periodontal tissues become flexible at the end of tooth movement, indicating reduced support by the periodontal tissues. Reitan26 reported that the collagenous fibers of the gingiva have reorganized normally within four to six months; on the other hand, the elastic supracrestal fibers remodeled more slowly and still could exert forces capable of displacing a tooth one year after removal of orthodontic appliances. The results of the current study were similar to those of Reitan.26
CONCLUSION
A longitudinal measurement of tooth mobility using the Periotest® protocol during two years following the removal of the orthodontic appliance was undertaken. The comparison of the relative mobility at appliance removal and at three-month intervals during the two years following appliance removal indicated that there was a rapid reduction in tooth mobility during the initial six months, a slower decrease after six months, and no significant decrease after twelve months. The results of the present study suggest that the early retention period, the first six months, is critical for stabilizing the periodontal tissue, and that mechanical retention is indispensable at least up to twelve months after orthodontic treatment.


 XML Download
XML Download