

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various treatment methods have been introduced for correction of anterior dental protrusion. Lingual appliances can contribute to efficiency while providing better esthetics during treatment.1,2 However, clinicians may be put off by high-priced brackets and complex mechanics in lingual treatment.3,4 These challenges are simplified with the combined use of a C lingual retractor and C plate for 3-dimensional control during anterior retraction.5 Since C plate acts as an independent retractor, without orthodontic appliances attached to the posterior teeth during en masse retraction, there is less risk of posterior periodontal problems arising (Fig 1).6,7 The authors refer to this treatment mechanic protocol as "Biocreative therapy", defined as independent en masse retraction of the anterior teeth while avoiding orthodontic appliances on the posterior segments during the retraction period.6,8 This alternative approach, which uses partially osseointegrated mini-implants or miniplates to resist multidirectional heavy forces can be beneficial in maximum anchorage cases that present with a poor dental health status, e.g. severe dental caries, advanced periodontal disease or missing teeth.
In patients with severe crowding, the lingual retractor is typically applied after leveling or decrowding. Otherwise the clinician may encounter premature contacts with the lower anterior teeth.
C-Plate combined lingual tube appliance
A unique appliance is used in substitution of fixed appliances on the upper posterior teeth. This consists of a stainless steel wire segment of 0.9 mm diameter with lingual tubes soldered to each end, which is wired to the extension arm of the C-plate and fixed with resin. The C-plate combined-lingual-tube appliance is placed in the midpalatal suture area (Fig 2) so that the lingual tubes are adjacent to the typical lingual molar tube. This provides a fixed anchor point for the retraction.
The clinical procedure of the C-plate combined lingual tube appliance is as following: 1. The C-plate is inserted in the midpalatal suture area followed with a pick up impression (Fig 2A); 2. The 0.9 mm stainless steel extension arm is bent and positioned to the stone cast (Fig 2B); 3. The 0.9 mm lingual tubes are soldered to the extension arm and adapted to the lateral C-plate arms (Fig 2C); 4. Resin material is applied to connect the extension arm to the C-plate arms (Fig 2D).
Specially designed labial brackets or lingual brackets can be used for effective decrowding of teeth into the extraction areas without any side-effects. The authors use either the labial bracket system (on the lingual) in 0.022-inch slot size (Delta force low friction appliance system, Ortho Organizers Inc., Carlsbad, CA, USA) or the 2-D lingual bracket system (Forestadent co., Pforzheim, Germany) for upper anterior decrowding and retraction (Fig 3). Most literature on lingual orthodontics seem to favor Kurtz brackets (Ormco Co., Orange, CA, USA) or Fujita brackets (Tomy Co., Tokyo, Japan) with excessive lingual root torque. However, the laboratory procedures for indirect bonding are complex, and the brackets are expensive. These brackets are designed to be easily ligated to the lingual area (unlike labial brackets). They have a triangular base which increases the contact area with teeth. However, we have been able to work well with relatively inexpensive labial brackets on the lingual surfaces of the anterior teeth. With the extension arm of the C-plate, 3-dimensional en masse retraction of the anterior teeth after decrowding can be attained with a single mini-plate inserted at the midpalatal suture area.
This case report describes the application of the modified lingual retractor and plate combination - a useful method for patients who need maximum anchorage, anterior torque control, and dental decrowding.
DIAGNOSIS AND ETIOLOGY
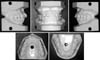
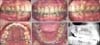
A 23-year-8-month-old female presented with a chief complaint of lip protrusion and a desire for a more esthetic smile. There was no remarkable medical history and temporomandibular joint function was normal. The pretreatment facial photographs revealed the facial characteristics typical of a bidentoalveolar protrusion patient with a short anterior facial height, prominent upper and lower lip, and convex profile (Fig 4). The pretreatment intraoral photographs and study models demonstrated Class II molar and canine relationships, a flat occlusal plane, and severely protruded and crowded incisors (Figs 4 and 5). The lower dental midline coincided with the facial midline and the upper dental midline was displaced 2 mm to the right. The cephalometric analysis showed a skeletal Class II relationship (ANB angle, 4.8°) with a slightly high mandibular plane angle (FMA, 30.8°) and protrusive lower incisors (Interincisal angle, 117.3°; Mandibular incisor to NA angle, 36.4°; Mandibular incisor to NB distance, 9.2 mm) (Fig 6A, Table 1). A low tongue posture was observed in the pretreatment lateral cephalometric radiograph. A panoramic radiograph revealed four impacted third molars (Fig 6B).
TREATMENT OBJECTIVES
The patient was diagnosed with Class II bi-dentoalveolar protrusion, and severe upper and lower anterior crowding She agreed to full retraction of upper and lower anterior teeth using first premolar extraction spaces and maxillary lingual orthodontic appliances. The treatment objectives, based on the results of cephalometric and study model analyses, were to make space with extraction of all the first premolars; decrowd and retract the anterior teeth; improve the interincisal angle relationship, decrease the lip protrusion, achieve a bilateral Class I canine and molar occlusion and improve the facial balance.
TREATMENT ALTERNATIVES
A treatment plan involving headgear for maximum anchorage was offered, but the patient declined this treatment option. Thus, two alternatives in the maxilla, both involving en masse retraction of the upper anterior dentition with temporary anchorage devices, were presented: (1) use conventional mini-implants in the palatal area as direct or indirect anchorage to reinforce the bonded or banded posterior anchorage teeth during anterior retraction, or (2) avoid placing posterior fixed appliances in the maxilla, and instead place a specially designed mini plate as an independent appliance for anterior retraction. The treatment plan to correct the lower crowding was presented as extracting both the lower first premolars with moderate anchorage management.
The second treatment plan for en masse retraction was selected. This plan allowed efficient decrowding and maximum retraction of upper anterior teeth without disturbing the molar occlusal relationships and minimizing stress on the periodontium. After en masse retraction of the upper and lower anterior teeth, full fixed appliances or tooth positioner would be used to finish the orthodontic treatment.
TREATMENT PROGRESS
For aligning of the 6 maxillary anterior teeth, we placed bicuspid brackets that are designed for the labial. These brackets have -12 degrees of torque, and 0 degree angulation. The brackets were placed with direct bonding. The upper right central incisor was bypassed at first. A 0.016 × 0.022-in stainless steel archwire was used for upper decrowding (Fig 7). The C-plate combined lingual tube appliance was applied immediately after C-plate placement. Aligning and en masse retraction of the lower anterior teeth were carried out with a 0.016 × 0.022-in NiTi archwire and 1/4-inch 3.5 oz Class I elastics.
Space was made for the blocked central incisor with open coil spring (Fig 8A). During anterior retraction, intrusion of lower anterior teeth was performed with a 0.019 × 0.025-inch stainless steel intrusion sectional archwire in the auxiliary tube of the lower first molar. Space for the upper right central was provided within 6 months and the tooth bracketed. Final decrowding was achieved with a 018 × 025-inch stainless steel archwire (Fig 8B). A 0.8 mm diameter stainless steel wire with hooks was soldered to the main arch wire between the central and lateral incisors to act as a lever arm to move the vector toward the center of resistance (Fig 8C).
The patient had an open bite tendency, and the goal was to retract with controlled tipping, since the anteriors were proclined. The vector of the retraction force in this patient was similar to that of the force system for distal crown movement of the anterior teeth with extrusion in the study of Lim and Hong.9 A 0.018 × 0.025-inch stainless steel archwire with T loops was used for detailing of the lower teeth (Fig 9). Inflammation occurred around the C-plate during the course of treatment, however, it remained stable (Fig 9D). Active treatment with fixed appliances was 18 months, when all appliances, (including the C-plate assembly under local anesthesia) were removed, followed by a tooth positioner for 1 month. The inflamed soft tissue healed after one week. The retention was provided by upper and lower lingual bonded retainers and wraparound retainers during night time.
RESULTS
After treatment, the patient obtained a Class I canine relationship (not solid on the right side) and a Class I molar relationship with coincidence of facial midline and dental midlines, improved overjet and overbite, corrected tooth position, proper alignment, and improvement in facial esthetics (Fig 10). There was slight residual space between the upper left canine and second premolar as well as minor scar tissue in the midpalatal area.
Cephalometric analysis (Figs 11A and 12, Table 1) showed a slight decrease of FMA (30.8°→30.1°). The occlusal plane increased during treatment due to controlled tipping of the upper anterior teeth and lower anterior intrusion (SN to OP angle, 19.3° to 25.6°). Both the upper and lower incisors were remarkably retracted (FH-U1 angle, 113.4° to 100.9°; Maxillary incisor to NA distance, 6.1 mm to 2 mm and the Maxillary incisor to NA angle, 21.5° to 10.1°; Mandibular incisor to NB distance, 9.2 mm to 5.9 mm and the Mandibular incisor to NB angle, 36.4° to 28.9°). The lower incisors were intruded and retracted (IMPA, 98.6° to 93.1°; FMIA, 50.6° to 56.8°). The lower lip in repose was more competent than the upper lip (UL to E-plane, 3.2 mm to 3.0 mm; LL to E-plane, 6.5 mm to 4.9 mm). The interincisal angle was increased from 117.3° to 135.9°. The posterior facial height/anterior facial height ratio increased a little after treatment (63.8% to 64.9%). The panoramic radiographs showed that root parallelism was attained and there were no evidence of root resorption (Fig 11B). The patient was pleased with the final treatment result. The 1 year retention intraoral photographs showed maintenance of the treatment results (Fig 13).
DISCUSSION
Many studies have described orthodontic implants for rigid anchorage and evaluated the effects of skeletal anchorage on dental and skeletal structures.10-12 Previous studies have consistently shown greater posttreatment changes in the implant anchorage group than the headgear group.13-15 Deguchi et al.14 compared the effect of incisor intrusion, force vector, and the amount of root resorption between the use of eight implant cases vs. 10 J-hook headgear patients. The result showed significantly greater reductions in overbite, maxillary incisor to palatal plane, and maxillary incisor to upper lip in the implant group than in the J-hook group. Lai et al.15 also showed that both skeletal anchorage groups had greater incisor retraction (6.9 mm using miniscrew, 7.3 mm using miniplate, 5.5 mm using headgear). They also reported that significant intrusion of the maxillary posterior teeth was noted in the miniplate group but not in the miniscrew and headgear groups.
However, studies of treatment results using lingual appliances combined with skeletal anchorage are limited.16,17 Chaushu et al.16 reported the lingual orthodontic treatment of an adult with an impacted maxillary canine, but their descriptions omitted the results of cephalometric and dental analyses. In spite of lingual appliance treatment being favorable to adult patients in terms of efficiency and esthetics, it is considered more difficult to achieve optimal outcome.
There are several differences in the choice of biomechanics between lingual and labial appliances.9,17 Using lingual appliances to retract incisors requires more attention to torque control since the force application is further away from the center of resistance of the incisors. With the labial appliance, it is awkward to apply a force vector close to the center of resistance because of the limitation imposed by anatomic structures. The force system required for lingual appliance therapy causes incisors to tip lingually to a larger degree. However, the Biocreative system with lingual appliances does not extend the treatment period compared with other conventional appliances.6,7
The aim of "Biocreative therapy", which consists of the en masse retraction of six anterior teeth, is to consider this segment as a whole and apply careful torque control during retraction.8 The C-plate combined lingual tube appliance enables a favorable outcome by achieving the treatment goals without any compromise. There are advantages of treating anterior bidentoalveolar protrusion by using the Biocreative therapy.8
First and foremost, the C-plate combined lingual tube appliance provides effective and safe anchorage for retraction of upper anterior teeth without posterior fixed attachments. As an absolute anchorage, it produces no reactive forces or negative side effects to the adjacent teeth. Chen et al.18 studied 359 skeletal anchorage systems (miniplates, miniscrews, and microscrews) in 129 patients to evaluate the clinical factors that influence the failure rates. They showed that the miniplate system has greater stability when compared with mini-implants. They concluded that mini-implants placed in younger patients or placed on the mandibular arch are at greater risk of failure. Second, alignment, intrusion and torque control are all achieved simultaneously with en masse retraction, which significantly shortens treatment time. Third, the specially designed bracket systems for C- plate combined retraction protocol facilitate correction of severe protrusion and crowding.
The midpalatal suture is as stable as other forms of skeletal anchorage systems, even when compared to extraoral auxiliares such as traditional biomechanical techniques.19 The clinical concerns with miniplates are not their stability or effectiveness, but rather the morbidity of flap surgery during insertion and removal of the miniscrews.20 In our studies, the palatal miniplate application without flap operations was as simple as a miniscrew application, even though the soft tissue around the C-plate showed mild swelling, but without severe complications. In contrast, microscrews have advantages: such as simple placement, less discomfort after insertion, and immediate loading. However, miniscrews have biomechanical limitations that affect design of force application.21
In the case reported here, while the upper posterior teeth were not used as anchorage teeth during en masse retraction, a slight mesial movement of the upper molars was observed in the cephalometric superimposition (Fig 12). This was insignificant compared to the amount of anchorage loss with conventional treatment mechanics. The authors suggest that minimal physiologic drifting may be positive for the closure of extraction spaces with force application in cases of Biocreative therapy. However, this patient showed insufficient anteriorretraction of lower dentition due to dental anchorages and also showed molar extrusion tendency after treatment. It was assumed to failure in vertical control in lower dentition during en masse retraction. We should have applied additional temporary skeletal anchorage devices in the lower dentition for anchorage control. To obtain an evidence-based conclusion and validate the effectiveness of lingual Biocreative therapy, further studies are required. This will add to knowledge of the long-term stability of treatment results by Biocreative therapy in comparison to other procedures for bidentoalveolar protrusion correction, as well as aid in understanding patient satisfaction and cost analysis.
CONCLUSION
1. Application of multiple self drilling miniscrews for a main source of retention allowed the C-plate to withstand multidirectional heavy forces from extended lingual sheath devices for anterior retraction.
2. Further research and studies on lingual Biocreative therapy orthodontic treatment mechanics will simplify application methods, enhance knowledge of detailing demands, and determine long term stability.












 XML Download
XML Download