

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Skeletal Class III malocclusion occurs because of an undergrowth of the maxilla, an overgrowth of the mandible, or both.1-5 Orthopedic treatment has been used to prevent the skeletal problems associated with this condition from becoming more severe, to eliminate or reduce the need for orthognathic surgery, and to improve the psychosocial well-being and appearance of the patient.6-8
Facemask with rapid maxillary expansion (FM/RME) or chin cup (CC) therapy has been used to treat growing patients with skeletal Class III malocclusion based on the cause of the skeletal discrepancy. Previous studies that have investigated the effects of FM/RME have reported forward movement of point A, counterclockwise rotation of the palatal plane, extrusion of the upper molars, labioversion of the maxillary incisors, and eventual clockwise rotation of the mandible.4,8-18 However, CC therapy has been shown to induce clockwise rotation and/or distal displacement of the mandible, to redirect mandibular growth vertically, and to remodel the mandible with closure of the gonial angle.16,19-24
Although several studies have evaluated the long-term craniofacial changes that occur as a result of using either of these orthopedic approaches,4,8,16,20,23-28 there have been few studies to date that have directly compared treatment effects between FM/RME and CC therapy.29 To precisely compare the treatment effects of these appliances, a confined set of patients that have both similar skeletal and dental patterns prior to orthopedic treatment and good retention results after fixed orthodontic treatment are necessary. Therefore, the purpose of this retrospective study was to compare the longitudinal treatment effects of FM/RME and CC therapy followed by comprehensive fixed orthodontic treatment in patients with skeletal Class III malocclusion.
MATERIAL AND METHODS
The samples consisted of twenty-one patients with Class III malocclusion who had similar skeletal and dental patterns, were treated by Delaire type FM/RME or Occipital pull CC, and exhibited good retention results after comprehensive fixed orthodontic treatment (approximately 5 years after the end of FM/RME or CC therapy). The criteria for good retention results consisted of a Class I canine and molar relationship, positive overbite and overjet, and a pleasing facial profile.
The patients were allocated into Group 1 (FM/RME, n = 11, 6 girls and 5 boys; mean age = 10.4 ± 1.5 years) and Group 2 (CC, n = 10, 5 girls and 5 boys; mean age = 9.9 ± 1.0 years) based on the treatment method they received. For both groups, the orthopedic appliances were used for at least 12 to 14 hours per day with a force of 300 to 500 g per side. After a 2 to 3 mm overbite and overjet was obtained, all subjects were treated with a straight archwire appliance (MBT set-up, 0.022'' slot, 3M-Unitek, Monrovia, CA, USA). During that period the orthopedic treatment was not accompanied. In Group 1, eight patients were treated with nonextraction and three with premolar extraction, while in Group 2, five were treated with nonextraction and five with premolar extraction. Fixed lingual retainers and removable circumferential retainers were also used.
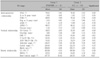
Lateral cephalograms with centric occlusion, reposed lip, and natural head position were taken before (T0) and after FM/RME or CC therapy (T1), and after fixed orthodontic treatment and retention (T2). The cephalometric variables are listed in Table 1. Cephalometric tracing and measurements were performed by one investigator using a digitizer (Intuos2 graphic tablet, Wacom Technology Co, Vancouver, Canada) and V-Ceph software (CyberMed, Seoul, Korea) at units of 0.05 degrees and 0.05 mm. Five randomly selected sets of cephalograms were retraced and redigitized after 2 weeks to determine the level of error in the initial measurements. There was no significant difference between the measurements (Dahlberg's formula, error of the linear measurement < 0.94 mm; error of the angular measurement < 1.05°), and thus the initial measurements were used for this study.
For statistical analysis, the program SPSS for Windows version 14 (SPSS Inc., Chicago, IL, USA) was used. Wilcoxon signed rank test was used to determine the difference between T0 and T1 stages and between T1 and T2 stages within the same group. Mann-Whitney test was used to compare the differences between Groups 1 and 2 during orthopedic therapy (T0-T1) and fixed orthodontic treatment and retention (T1-T2).
RESULTS
Comparison of the mean age according to the stage between Groups 1 and 2 (Table 2)
There was no significant difference in age at each stage between Groups 1 and 2, indicating that the samples were matched in terms of age. The mean durations of the orthopedic treatment with the FM/RME and CC therapies were 1.4 and 2.0 years, respectively. The mean durations of the fixed orthodontic treatment and retention for Groups 1 and 2 were 5.1 and 5.2 years, respectively.
Comparison of the skeletal and dental variables prior to FM/RME and CC therapy between Groups 1 and 2 (Table 3)
There was no significant difference in the skeletal and dental variables at T0 stage between Groups 1 and 2 except interincisal angle (larger in Group 1, p < 0.05). These findings imply that the samples were well matched in terms of their skeletal and dental variables.
Comparison of the skeletal and dental changes during FM/RME and CC therapy in each group (Table 4)
In the anteroposterior position of the maxilla, there was significant forward movement in Group 1 (A to N perp, p < 0.05), but not in Group 2, as expected. In the anteroposterior position of the mandible, both groups exhibited significant posterior repositioning of the mandible (SNB, p < 0.01; Pog to N perp, p < 0.01; APDI, p < 0.01; ANB, p < 0.01, both respectively). In addition, Group 1 showed a more significant improvement in overjet (p < 0.01) due to labioversion of the upper incisors (p < 0.01).
Regarding changes in the vertical relationship, there was a significant increase of SN-GoGn (p < 0.01), ANS-Me/N-Me (p < 0.01), and Björk sum (p < 0.01), as well as decrease of overbite (p < 0.05) in Group 1, and a significant increase in articular angle (p < 0.05) and decrease in gonial angle (p < 0.01) in Group 2.
There was a significant decrease in interincisal angle (p < 0.05) due to significant labioversion of the upper incisors in Group 1 (p < 0.01); however, there were no significant changes in inclination of the lower incisors of Group 1, nor the upper and lower incisors of Group 2.
Comparison of changes in the skeletal and dental variables during FM/RME and CC therapy between Groups 1 and 2 (Table 4)
There was no significant difference in the amount of change in the anteroposterior positions of the maxilla and the mandible between Groups 1 and 2; however, Group 1 did exhibit a significant increase in overjet compared to Group 2 (p < 0.05).
Regarding changes in the vertical relationship, there were significant differences in the amount of change in ANS-Me/N-Me (p < 0.01), SN-GoGn (p < 0.05), Björk sum (p < 0.05), and gonial angle (p < 0.05) between Groups 1 and 2. These findings suggest that FM/RME and CC therapy may exert different effects on the vertical dimension in cases with successful results.
There were no significant differences in the amount of change of the dental variables between Groups 1 and 2.
Comparison of changes in the skeletal and dental variables during fixed orthodontic treatment and retention in each group (Table 5)
For the anteroposterior position of the maxilla and the mandible, both groups showed significant forward growth of point A (A to N perp, p < 0.05, respectively). Although both groups revealed statistically significant deterioration of overjet (p < 0.01 in Group 1, p < 0.05 in Group 2), significant forward repositioning and growth of the mandible (Pog to N perp, p < 0.01) was observed in Group 1 only.
In the vertical relationship, there was a significant counterclockwise rotation of the mandible (decrease of SN-GoGn and Björk sum, p < 0.05, respectively) in Group 1; however, Group 2 had a significantly increased lower anterior facial height (ANS-Me/N-Me, p < 0.01) and decreased overbite (p < 0.05). These findings indicate that there may be a different tendency of change in vertical dimension between Groups 1 and 2 during T1-T2 phase.
In Group 1, although there was no significant change in inclination of the upper incisors, the lower incisors were significantly labially inclined (IMPA, p < 0.05). There was no difference in inclination of the upper and lower incisors for Group 2.
Comparison of changes in the skeletal and dental variables during fixed orthodontic treatment and retention between Groups 1 and 2 (Table 5)
There was no significant difference in the amount of change in the anteroposterior position of point A and the mandible between Groups 1 and 2. In the vertical relationship, Group 2 exhibited a significant increase in ANS-Me/N-Me (p < 0.05) compared to Group 1, while Group 1 exhibited a significant increase in IMPA (p < 0.05) compared to Group 2.
DISCUSSION
Skeletal and dental variables before FM/RME and CC therapy (T0)
Results of the orthopedic and orthodontic treatments, as well as growth of the maxilla and mandible, can be affected by original skeletal and dental characteristics.22,24,30 In this study, at T0 stage, there were no significant differences in the anteroposterior position and vertical dimension of the maxilla and mandible between Groups 1 and 2 (Table 3). Therefore, both groups appeared to have similar skeletal characteristics for Class III malocclusion prior to orthopedic treatment.
FM/RME group had a greater interincisal angle (p < 0.05, Table 3) because of a greater lingual inclination tendency of the upper incisor than CC group, although this difference was not statistically significant. Since Class III malocclusion patients with severe compensated upper and lower incisors, vertical growth pattern, and prognathic mandible would be one of the contraindication of FM/RME and CC therapy, these types of patients were excluded from initial sampling. Uçüncü et al.29 reported that there were significant differences in the position of the upper incisor between FM/RME and CC groups at T0 stage. In this study, lingual inclination of the upper incisors with retruded maxilla could be a good indicator for determining FM/ RME therapy or CC therapy.
Changes in the skeletal and dental variables during FM/RME and CC therapy (T0-T1)
Regarding the amount of change in the anteroposterior position of the maxilla, there was a significant forward movement of the maxilla (A to N perp, p < 0.05, Table 4) in FM/RME group, which was expected based on the results of previous studies.4,8,9,12,16,31,32 CC group did not show a significant forward movement of the maxilla (Table 4), which was also in accordance with other studies;19,21,33,34 however, the finding that there was no significant difference in the amount of change of point A between groups 1 and 2 during T0-T1 (Table 4) indicates that forward growth of the maxilla could have occurred after correction of the anterior crossbite in CC group, although the extent to which this occurred was less than FM/RME group. Also no significant difference in the amount of change of point A between Groups 1 and 2 may be due to the difference of treatment duration between groups 1 and 2.
In the present study, both FM/RME and CC groups showed significant improvement in their sagittal skeletal discrepancy (SNB, Pog to N perp, ANB, APDI; p < 0.01, Table 4), which was consistent with other studies.5,8,9,12,14,16,25,29,35 In addition, FM/RME therapy induced more significant improvement of overjet (p < 0.05, Table 4) compared to CC group during T0-T1, which was attributed to significant forward movement of the maxilla and labioversion of the upper incisors of FM/RME group (A to N perp, p < 0.05; U1-SN, p < 0.01; Table 4).
With respect to the vertical relationship, FM/RME group exhibited more significant clockwise rotation of the mandible than did CC group (SN-GoGn, Björk sum, ANS-Me/N-Me, p < 0.01, Table 4). These findings indicate that FM/RME caused a significant increase in vertical dimension, while CC might have had a remodeling effect on the mandible. Consistent with this finding, Uçüncü et al.29 and Arman et al.16 reported that there was significant clockwise rotation of the mandible during FM therapy.
Although CC therapy is known to cause significant clockwise rotation of the mandible,19-23 CC group in this study, which had good orthopedic treatment results, did not exhibit the same outcome, which is in accordance with Ko et al.,24 who, after performing a long term study of CC therapy, reported that the group with poorest retention results showed more clockwise rotation than the group with good retention results. Mitani and Sakamoto36 insisted that retardation of the forward growth of the chin during chincup treatment was dependent upon a reduction of the growth increment of mandibular length and a decrease in gonial angle in addition to distal displacement of the mandible. Therefore, a decrease in gonial angle (p < 0.01, Table 4), labioversion of the upper incisor, and linguoversion of the lower incisors could all have contributed to increase of overjet observed with CC therapy in this study.
Changes in the skeletal and dental variables after fixed orthodontic treatment and retention (T1-T2)
With respect to the forward growth of the maxilla and mandible in Class III malocclusion patients after orthopedic treatment, previous studies have shown that, after FM/RME therapy, the maxilla grows the same as untreated Class III malocclusion patients, but less than Class I malocclusion patients, and that the amount of mandibular growth was similar among these groups.13,15,27 Wisth et al.37 reported that changes of the maxilla and mandible in patients treated with FM and quad-helix were not significantly different from Class I malocclusion controls.
Numerous studies19,20,25,36 have reported that catch-up growth of the mandible in the forward direction after CC therapy resulted in return to the original skeletal morphology and growth pattern. However, Deguchi et al.23 insisted that changes in the sagittal maxillary and mandibular relationship by CC therapy remained stable after fixed orthodontic treatment and retention. Ko et al.24 reported on the basis of a long term study of Class III malocclusion patients with CC therapy, that patients with the poor retention results had more counterclockwise rotation and forward growth of the mandible compared with patients who had good retention results.
When compared to the changes in point A to N perp with Pog to N perp between Groups 1 and 2 (1.47 mm vs 4.43 mm and 0.88 mm vs 2.77 mm, respectively, Table 5), the net differences were 2.96 mm and 1.89 mm, respectively. This finding suggests that although the skeletal characteristics of Class III malocclusion might recur to a certain degree during T1-T2, there was significant forward growth of the maxilla in both groups (p < 0.05, respectively, Table 5). Considering the chronological age of the patients at the T2 stage, there was likely very little remaining mandibular growth potential, especially in girls. To evaluate the end of active skeletal growth, the skeletal age such as hand-wrist and cervical vertebral maturation index method would be needed.
The finding of a significant decrease in SN-GoGn and Björk sum in Group 1 (p < 0.05, respectively, Table 5) and increase in S-Go/N-Me in Group 2 (p < 0.05, Table 5) indicates that the mandible rotated counterclockwise due to relapse and continued growth of the mandible. In addition, Group 2 exhibited a significantly increase of lower facial height ratio (ANSMe/N-Me, p < 0.01, Table 5), which was in accordance with the findings of Ko et al.24
The significantly decreased overjet in Group 1 (p < 0.01, Table 5) appeared to be due to the significant labioversion of the lower incisors (p < 0.05, Table 5) and counterclockwise rotation and growth of the mandible (SN-GoGn, Björk sum, p < 0.05, respectively, Table 5).
There are some limitations of this study such as small sample size, sexual dimorphism of subjects, use of the chronological age, and need of untreated Class III or Class I malocclusion as control groups.
CONCLUSION
1. FM/RME and CC therapy produced a different spectrum of effects on skeletal and dental components.
2. The key factor for successful FM/RME and CC therapy and good retention results might be a harmonized forward growth of the maxilla that could keep pace with the growth and rotation of the mandible.




 XML Download
XML Download