

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bimaxillary dental protrusion is considered to be a subclass of Class I malocclusion, showing normal molar relationships, normal overbite and overjet and anterior inclinations of the maxillary and mandibular incisors.1-3 Bimaxillary dental protrusion, with accompanying lip protrusion or lip sealing incompetency, results in unaesthetic facial profiles. Cox and van der Linden4 reported that persons with poor facial esthetics generally have a relatively more convex face due to anterior positioning of the midface, including the teeth. Keating5 reported the morphological features of bimaxillary protrusion in a cephalometric study. McCann and Burden6 used dental casts of bimaxillary protrusions according to Keating's criteria and found a correlation between tooth size and bimaxillary dental protrusion.
Dental crowding is defined as a disharmony in the available basal arch length and the required arch length of age and gender in the samples for proper alignment of the teeth.7,8 Doris et al.9 defined crowded arches as those with more than a 4 mm space deficiency, and reported that all of the teeth in the crowded group were uniformly larger than in the good alignment group.
A review of the literature regarding bimaxillary dental protrusion6 and dental crowding9,10 reveals that both types of malocclusions have larger teeth than normal; however, their tooth alignment and facial profiles show different patterns. These findings indicate that other factors might determine dental protrusion or dental crowding in an individual with large tooth size.
On the other hand, many etiologic factors have been suggested for the development of dental protrusion such as low lip force, mouth breathing, large tongue, and tongue thrusting habits.11-14 However, few studies have directly compared dental protrusion with dental crowding. This study was performed to investigate the differences in the lateral cephalometric characteristics between dental protrusion and crowding and to determine the etiology of each type of malocclusion.
MATERIAL AND METHODS
Subjects
The sample in this study was selected from the orthodontic patient record of a university hospital. For the first step, patients with larger than average teeth were selected, on the basis of the four mandibular incisors, as both dental protrusion and dental crowding are found in patients with large teeth.6,9,10 The sum of the four mandibular incisors was required to be larger than the average (males 22.8 mm, females 22.0 mm).15 Any subject who presented Class II or Class III was excluded. The patients were also limited to those over 18 years of age.
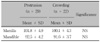
The final step in the sample selection for the dental protrusion group was to investigate cephalometric measurements. The patients were restricted to those satisfying the criteria of Keating's study;5 a maxillary incisor angle over 115°, mandibular incisor angle over 99°, and an interincisal angle under 125°. For the dental crowding group, they were required to have an arch length discrepancy over 4 mm in both the maxillary and mandibular arches.9 Twenty nine subjects with dental protrusion and 22 subjects with dental crowding were selected from 4,500 patient records (Table 1).
Measurement and comparison of tooth size
Patients with dental protrusion or dental crowding with large teeth were selected based on the dimensions of their mandibular incisors. However, this did not mean that all teeth were of equal sizes in the two groups. In order to confirm size, the mesiodistal diameters of 12 teeth, from the central incisor to the first molar of both sides in one arch and again in the other arch, were measured using a digital vernier caliper. Then, the sums of all of the measured values of the maxillary arch and the mandibular arch were compared between the two groups.
Tracing and measurement of lateral cephalometric radiographs
Lateral cephalograms were traced and 16 skeletal landmarks, 4 dental landmarks, and 8 cervical and hyoid bone landmarks were designated as shown in Fig 1. The measurements reflecting the craniofacial characteristics, the incisor positions, and the positions of the hyoid bones were defined on each tracing. The measurements of hyoid bone positions were determined as shown in Fig 2.
Statistical analysis
SPSS software (SPSS for windows version 12.0, Chicago, Il, USA) was used for the calculation of means and standard deviations of all the measurements, and independent t-tests were used to determine significant differences between the two groups. A p-value < 0.05 was considered significant.
RESULTS
Tooth size comparison
A comparison of the sum of the mesiodistal diameters from the central incisor to the first molar showed no significant differences between the two groups in either the maxillary or the mandibular dentitions (Table 2).
Comparison of craniofacial measurements
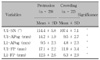
Comparisons of the craniofacial measurements revealed significant differences between the two groups in five of seventeen measurements: S-N, A'-Ptm', SNA, ANB and facial convexity. All these measurements showed greater values in the protrusion group than in the crowding group, indicating that the patients with dental protrusion have a larger cranial base, longer maxillary length, and greater facial convexity compared to the patients with dental crowding (Table 3).
Comparison of the position of incisors
The measurements of U1-SN, U1-APo, L1-APo, U1-FP and L1-FP showed that all of these measures were greater in the protrusion group, and hence confirmed that the upper and lower incisors in the protrusion patients were more anteriorly positioned than in the crowding patients (Table 4).
Comparison of the position of the hyoid bone
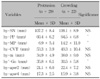
In the comparisons of the hyoid bone measurements, significant differences were observed for hy-PP, hy-MP and hy'-Go. The measurements for hy-PP and hy-MP showed smaller values in the protrusion group indicating that the position of the hyoid bone was placed more superior in the protrusion group than in the crowding group. For hy'-Go, it showed a greater value in the protrusion group indicating that the hyoid bone was located more anteriorly in the protrusion group than in the crowding group (Table 5).
DISCUSSION
A review of the literature indicates that dental protrusion is caused by large tooth size.9,10 The results of tooth size measurement in the present study showed that the tooth size for the protrusion group was greater than that of normal occlusion individuals.15 However, there was no significant difference in tooth size between the protrusion group and the crowding group in this study; dental crowding is also caused by large tooth size. These findings indicate that tooth size is not the sole factor that determines dental protrusion. When an individual has larger teeth than normal, he or she might develop into dental protrusion or dental crowding according to some other factors. The purpose of the present study was to investigate the differences in the lateral cephalometric characteristics between dental protrusion and crowding in order to determine what factors affect dental protrusion or crowding while both types of malocclusions are caused by large tooth size.
In order to draw meaningful conclusions, the matter of sample selection is of utmost importance. The sample for this study was selected from the orthodontic patient records of a university hospital. For the first step, the patients with larger than average teeth were selected because both dental protrusion and dental crowding are found in patients with large teeth.6,9,10 The sizes of the four mandibular incisors were used as the inclusion criteria for the selection of patients since they are known to be relatively stable, whereas the maxillary incisors show variability in sizes.16,17 The sum of the mesiodistal diameters was required to be larger than average.15 In addition, subjects with Class I molar relationships were included; any subject who presented Class II or Class III was excluded because accurate comparisons of lateral cephalometric measurements were not possible for these subjects. The patients were also limited to those over 18 years of age in order to compare differences after growth was complete. Finally, the subjects were restricted to those satisfying the cephalometric criteria of Keating's study for the dental protrusion group.5 As for the dental crowding group, they were required to have an arch length discrepancy over 4 mm in both the maxillary and mandibular arches.9 Twenty nine subjects with dental protrusion and 22 subjects with dental crowding were selected as the sample for the study. Substantial efforts were required to select these numbers of the sample; 4,500 consecutive patient records were used for the sample selection of the present study.
In the comparisons of craniofacial measurements, there were significant differences between the protrusion and crowding groups for S-N, A'-Ptm', SNA, ANB and facial convexity. These measurements were greater in the protrusion group, indicating that the patients with dental protrusion had a larger cranial base, longer maxillary length and greater facial convexity compared to the crowding individuals. Keating5 reported similar number of values for A'-Ptm' (50.7 mm), SNA (82.3°), and ANB (9.7°) in his study regarding bimaxillary protrusion. The results of that study indicated that dental protrusion would develop in cases of maxillary protrusion. Considering that only Class I subjects were used in this study, a skeletal Class II tendency is a contributing factor to dental protrusion, even in an individual with a Class I molar relationship. On the other hand, Rose and Roblee18 maintained, in a recent review, that alveolar bone discrepancies should be considered as a leading cause of dental crowding. They further insisted that treatment should focus on the development of alveolar bone to relieve crowding. Their study suggests that dental crowding is developed in case of bone deficiency.
It is also interesting to note that the measurements for S-N showed greater values in the protrusion group. Considering that the measurements for facial convexity also presented greater values in the protrusion group, it is suggested that the size of the craniofacial skeleton is greater in the protrusion group than in the crowding group. These results indicate that the size of the craniofacial skeleton might be a determining factor for dental protrusion or dental crowding.
As soft tissue components have been reported to be related to the development of dental protrusion in addition to skeletal features,11-14 investigation of tongue position was needed. Considering that tongue position is influenced by the position of the hyoid bone,19,20 the measurements indicating the hyoid bone position were defined in this study. It has been reported that hyoid position might be influenced by many factors: the supra- and infra-hyoid muscles,19-21 head posture21,22 and craniocervical posture.23,24 With this in mind, particular attention was paid to defining the measurements reflecting hyoid bone position in this study. The measurements of hy-SN and hy-PP were established to reflect the hyoid position on the basis of the cranium and nasomaxillary complex, whereas the hy-MP and hy'-Go were defined on the basis of the mandible. The measurements of hy-apw2 and hy-apw4 were established based on the anterior pharyngeal wall. In addition, hy-CVT was defined on the basis of the cervical column according to Carlsoo and Leijon25 who reported that determination of hyoid position using the cervical column as a reference was more valid than using the cranium or mandible.
Comparisons of the hyoid bone measurements between the two groups showed that the hyoid bone was positioned more superiorly and anteriorly in the protrusion group than in the crowding group. These results indicate that a difference in the hyoid position might have an effect on the determination of whether dental protrusion or crowding develops. Considering that hyoid position influences the position of the tongue,19,20 this suggests that tongue position or pressure affects whether dental protrusion or crowding develops in an individual with large tooth size.
Overall, the findings of this study are that the protrusion group showed a larger cranial base, longer maxillary length, greater facial convexity and a tendency for an antero-superior position of the hyoid bone compared to the crowding group. These results indicate that dental protrusion or crowding might be determined according to maxillary growth and tongue position when an individual has larger teeth than normal. However, the exact cause-effect relationship could not be elucidated in the present study. The above characteristics might be the results of dental protrusion or crowding, but not necessarily the causes. Additional studies to investigate these relationships should be conducted.
On the other hand, Angle's classification alone was used as an inclusion criteria while Class I subjects were used as the sample for both groups in the present study. Considering that Class I subjects might show Class II or III in terms of skeletal characteristics, it would be interesting to investigate the hyoid bone position of the dental protrusion or crowding individuals with skeletal Class I as well as dental Class I characteristics.
CONCLUSION
Comparisons of the cephalometric characteristics showed that the protrusion group showed a larger cranial base, longer maxillary length, greater facial convexity and a tendency of an antero-superior position of the hyoid bone compared to the crowding group. These results indicate that some cephalometric characteristics could be determining factors for whether dental protrusion or crowding develops; when an individual has large teeth, dental protrusion or crowding might be determined according to maxillary growth and tongue position.




 XML Download
XML Download