

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nasal breathing is the primary mode of air intake for the human, and it is essential for a supply of properly cleansed, moistened and warmed air for the lungs.1 It is the first physiological function developed at birth and serves as protection for the respiratory tract, and also plays a fundamental role in the development of facial morphology.2 On the other hand, oral breathing can interfere with the craniofacial growth of the developing child and alter dentofacial morphology and have negative effects on cognitive and psychosocial development. It can also lead to maxillary atrophy, dental protrusion, and excessive vertical growth, which is undesirable in dolichocephalic patients.
Oral respiration associated with an obstructed nasal airway is common in orthodontic patients. Oral respiration and a nasal airway obstruction is associated with a variety of skeletal-dental problems.3 Mouth breathing has long been assumed to influence the facial form, and in particular, predispose the patient to the development of "long face syndrome" or "adenoid facies".4 Ricketts5 lists the characteristics of respiratory obstruction syndrome as a cross-bite, the presence of enlarged tonsils or adenoids, or a history of respiratory problems, open-bite, tongue-thrust upon swallowing and mouth-breathing. Other findings include an excessive anterior facial height, incompetent lip posture, excessive appearance of the maxillary anterior teeth, narrow external nares, steep mandibular plane angle, and a "V" shaped maxillary arch.
Correction of transverse maxillary width discrepancies by opening of the midpalatal suture has been an integral part of orthodontic therapy for many years. Rapid maxillary expansion (RME) has been recommended for the correction of maxillary transverse deficiency with the additional benefit of increasing nasal airflow.6-9 Evidence to support this comes both from patients' self-reported perceptions and from radiographic images.
In children and adolescents, conventional orthodontic RME has been successful when used prior to sutural closure. On the other hand, in skeletally mature patients, the possibility of successful maxillary expansion decreases as the sutures close and the resistance to mechanical force increases. After sutural closure or the completion of transverse growth, orthopedic transverse maxillary expansion is largely unsuccessful because the expansion is composed primarily of alveolar or dental tipping with little or no basal skeletal movement.10
In mature patients, RME also causes severe pain, periodontal complications, and gingival recession of the maxillary posterior teeth. Surgically-assisted RME (SARME) has been proposed to produce better treatment results in adults as well as to prevent complications by surgically releasing the closed sutures resisting the expansion forces.10 The SARME procedure decreases the risk of aseptic necrosis and relapse, particularly in patients with a major transverse discrepancy. SARME is a useful and predictable technique for achieving transverse maxillary expansion.11
As above-mentioned, RME increases the transverse dimension of the maxillary arch by separating the suture. However, mandibular expansion effects are localized to the alveolar bone and primarily induce tooth inclination. These effects are believed to be related to relapse.12-14 The addition of a lower Schwarz appliance to the treatment protocol allows significant extrusion of the lower molars and incisors. These changes correlate with the increase in vertical skeletal dimension.15
Surgical superior impaction of the maxilla has become an accepted treatment for the correction of vertical maxillary excess. Orthognathic surgery, which vertically repositions the maxilla, does predictably reduce nasal resistance, which intuitively should increase the percentage of nasal flow.16
On the other hand, directional force technology reinforced with MIA (microimplant anchorage)17 is a useful treatment approach for correcting a Class I or Class II dentoalveolar protrusion malocclusion. In particular, it is effective in treating patients with vertical problems, such as clockwise rotation of the dentoalveolar complex. In addition, it can create a favorable counterclockwise skeletal change as well as a balanced face minimizing surgical treatment.17,18
DIAGNOSIS AND ETIOLOGY
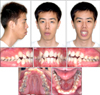
A 22-year-old male presented with the chief complaint of lip protrusion and difficulty in nasal breathing. Facially, he exhibited a convex profile due to a retrognathic mandible. The facial photographs showed a convex facial profile with marked protrusion of the lips, mentalis strain, an excessive lower anterior facial height and a typical "adenoid face". Intraorally, he had a Class I canine and molar relationship with moderate crowding, severe constricted "V" shaped arch forms of both jaws, an anterior openbite and poor oral hygiene (Fig 1).
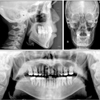
The panoramic radiograph revealed the presence of upper left and lower right third molars as well as restorations on several teeth. The lateral cephalogram and its tracing confirmed the severe skeletal problem (Fig 2). The skeletal pattern was deemed hyperdivergent as evidenced by a FMA (Frankfort-mandibular plane angle) of 33.5° and a FHI (facial height index) of 0.61%. The ANB angle of 4.5° reflected the class II skeletal problem. The Z-angle of 51.5° quantified the facial imbalance (Table 1). The posteroanterior cephalometric radiograph showed a 2-mm deviation of the mandibular dental midline to the left relative to the maxillary dental midline with slight canting of the maxilla and transverse contriction of upper and lower arches (Fig 2). There were no significant signs or symptoms of any temporomandibular disorders.
TREATMENT OBJECTIVES
The treatment objectives were to (1) align and level the teeth in both arches and establish a functional occlusion, (2) normalize the overjet and overbite relationships, (3) obtain a balanced facial profile, and (4) control the mouth breathing habit.
TREATMENT ALTERNATIVES
The first alternative was orthognathic surgery. Two-jaw surgery including counterclockwise differential impaction of the maxilla and concurrent mandibular advancement surgery would be followed after expanding both constricted arches. Genioplasty would be necessary to reduce the long lower facial height and advance the chin along the facial midline. However, the patient requested minimal surgery so another treatment plan was chosen.
The second alternative was expansion of the constricted upper and lower arches with SARME and a Schwarz appliance, respectively, followed by orthodontic treatment with extraction of the 4 first premolars and 2 third molars, and directional force technology with MIA. As described previously,17 MIA can provide absolute anchorage not only in the retraction of the maxillary and mandibular anterior teeth, but also in the intrusion of the maxillary anterior and posterior teeth, and mandibular posterior teeth. This would induce a horizontal mandibular response followed by a balanced facial profile.
TREATMENT PROGRESS
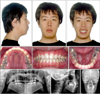
The protocol began with a phase I treatment in which the Schwarz appliance was activated once per week for approximately 5 months. SARME was followed concurrently with mandibular expansion. A Hyrax palatal expansion appliance was cemented to the maxillary first molars and first premolars. The patient was then referred to the oral surgery department for the surgically assisted expansion procedure. At the conclusion of surgery, the surgeon turned the expansion appliance until the papillary gingival tissue blanched between the central incisors (8 turns or approximately 2 mm). The patient returned to the orthodontic department 7 days later (Fig 3). The patient was instructed to turn the appliance two turns per day (0.5 mm) for 20 days and then 1 turn per week for a further 28 days until the desired level of expansion was achieved (Fig 4). After the expansion, a hyrax palatal expander remained in place for an additional 3.5 months while the mandibular expansion was completed (Fig 5).
The phase II treatment plan involved Tweed-Merrifield directional force technology with MIA, after extracting the maxillary and mandibular first premolars, as well as the third molars.
After the extractions, 0.022 × 0.028-in nontipped, nontorqued edgewise appliances were placed in both arches, and leveling began with a 0.014-in nickel-titanium archwire and 0.018 stainless steel arch wires. Maxillary posterior MIs (microimplants, 1.3 - 1.2 mm in diameter, 8 mm in length; Absoanchor SH1312-08, Dentos, Taegu, South Korea) were implanted into the buccal alveolar bone between the maxillary second premolars and first molars. The mandibular posterior MIs (1.3 - 1.2 mm in diameter, 7 mm in length; Absoanchor SH1312-08, Dentos) were implanted into the buccal alveolar bone between the mandibular first and second molars. An elastic chain force was loaded immediately after placing the MIs, from the maxillary and mandibular posterior MIs to the canine brackets, in order to retract the maxillary and mandibular canines to level the six anterior teeth (Fig 6A).
Two months into the treatment, 0.019 × 0.025-in stainless steel archwire with closing loops was placed in the lower arch to retract the six anterior teeth. An intruding force was applied from the mandibular posterior MIs to the omega stop loop areas of the mandibular archwire in order to prevent mesial tipping and extrusion of the mandibular posterior teeth. Three months into the treatment, a 0.017 × 0.022-in stainless steel archwire was placed in the upper arch to level the six anterior teeth and an intruding force was applied from the maxillary posterior MIs to the maxillary archwire to intrude the maxillary posterior teeth. An additional unilateral Class III elastic force was applied to the loop of the mandibular archwire from the maxillary posterior MIs in order to reduce the dental asymmetry (Fig 6B).
Four months into the treatment, 0.020 × 0.025-in stainless steel archwire with closing loops was placed in the upper arch to retract the six anterior teeth. This was supported by the maxillary anterior MIs (microimplants, 1.3 - 1.2 mm in diameter, 8 mm in length; Absoanchor SH1312-08, Dentos) that were implanted into the labial alveolar bone between the maxillary central incisors for torque control, bodily movement and intrusion of the maxillary anterior teeth (Fig 6C).
After en masse movement, directional force control was performed to promote a mandibular response. The treatment was completed with ideal archwires (0.020 × 0.025-in stainless steel archwire in the upper arch and 0.019 × 0.025-in stainless steel archwire in the lower arch) and cusp-seating elastics (Fig 6D). Fixed lingual retainers were bonded to the lingual sides of the six anterior teeth and circumferential clear retainers were placed on both arches, immediately before and after removing the appliances for retention, respectively. The total treatment time of phase II was 24 months.
RESULTS
At phase I of the treatment, considerable maxillary and mandibular expansion was achieved in the anterior and posterior segments, and the expansion provided the space to align the maxillary and mandibular anterior teeth. The posteroanterior cephalometric radiograph showed an increase in transverse dimension of intermolar width (measured from the buccal surface of the maxillary left first molar to the buccal surface of the maxillary right first molar) by 10.0 mm after 1 month expansion with SARME and an increase in transverse dimension of intermolar width in the mandibular arch by 5.5 mm after 5 months of expansion with the plane angle) was increased by 1° due to molar extrusion as a result of the expansion of both arches but was recovered during the retention period of phase I. The facial appearance was worsened slightly by the clockwise rotation of the mandible. However, the patient was pleased with the slightly peaceful looking facial appearance along with easier nasal breathing.
After phase II treatment, the post-treatment facial photographs (Fig 7) and lateral cephalometric radiograph (Fig 8) showed a well balanced and harmonious face through retraction of the upper and lower lips, reduction of the mentalis muscle strain, and decrease in the lower anterior facial height. The intrusive forces used on the maxillary anterior segment successfully reduced the excessive gingival display during smiling. The intraoral photograph showed good interdigitation of the teeth, an acceptable arch form and a normal overjet-overbite relationship (Fig 7). The post-treatment panoramic radiograph showed good overall root parallelism with no significant resorption of root and alveolar bone (Fig 8). The post-treatment posteroanterior cephalometric radiograph showed a coincident dental midline but a slight canting remained, and relapse of transverse dimension of the maxillary intermolar width by 5.5 mm and an additional increase of the mandibular width by 3.5 mm (Fig 8). The thirteen-month retention records showed good retention without any obvious relapse (Fig 9).
As shown on the pretreatment and post-treatment cephalometric superimposition (Fig 10A), the maxillary anterior teeth were bodily retracted with intrusion, the maxillary posterior teeth were intruded, the mandibular anterior teeth were retracted with uprighting, and the mandibular posterior teeth were uprighted. A good mandibular response was achieved through the counterclockwise directional forces. Chin advancement was obtained by autorotation of the mandible, which was facilitated by vertical control of the dentition, resulting in a 3.0° decrease in the Frankfort-mandibular plane angle, and a 1.5° reduction of the ANB angle. The mandibular incisors were uprighted from 93.0° to 76.5°. The Z-angle was improved from 51.5° to 61.5°, the Frankfort-mandibular incisor angle was increased by 19.5°, and the anterior facial height was reduced by 3 mm. All these changes contributed to improving the facial profile. The post-treatment and 13-month retention cephalometric superimposition (Fig 10B) showed slight relapse, such as extrusion of the posterior teeth, a 1.5° increase in the Frankfort-mandibular angle, a 0.5° increase in ANB angle, and 1 mm lengthening of the anterior facial height (Table 1).
DISCUSSION
The typical dental and morphological characteristics associated with nasal impairment have been reviewed in detail elsewhere and can be summarized as follows: an increase in the total anterior face height that is primarily due to a more vertical development of the lower anterior face. Concomitantly, an increase in the mandibular plane and gonial angles as well as tipping of the palate can be observed.2,19 Therefore, mouth breathing caused by a nasal airway obstruction must be considered a major etiological factor for the induction of excessive vertical growth.20
The causes3 of nasal obstruction followed by oral respiration can be adenoid or tonsil hypertrophy, nasal injury, congenital nasal deformities, foreign bodies, polyps, and neoplasms. Procedures, such as intranasal surgery, maxillary expansion, and medication for the control of mucosal swelling, are used to improve the airflow through the nose. The patient in this case report had undergone intranasal surgery several years ago earlier but the symptom had not improved.
The influence of an airway obstruction on the development pattern of the face is controversial. As shown in this patient, a nasopharyngeal obstruction could be associated with the downward and backward rotation of the mandible resulting in an anterior openbite and a long anterior facial height. On the other hand, Vig et al.16 reported that patients with a long vertical face height had higher nasal resistance than normal patients, however, these individuals did not necessarily have the lowest nasal airflow.
Rapid palatal expansion (RPE) has become an established, proven method for treating children and adolescents with severe transverse maxillary deficiencies combined with a crossbite. However, in adults, this technique is frequently associated with complications, such as buccal tipping, extrusions, root resorption and fenestrations of the alveolar process of the supporting teeth absorbing the force.21 Therefore, surgically assisted rapid palatal expansion (SARPE) is more likely to be considered for adults.
SARPE is a simple, effective and stable procedure for correcting severe maxillary transverse deficiencies.22,23 It not only increases the intermolar distance and palatal width but, in certain cases, can improve nasal respiration.6-9 Therefore, we decided to expand the maxilla with SARPE to increase the nasal airflow and recommended that he undergo nasal breathing exercises. However, this technique is occasionally associated with complications, such as devitalization of teeth and altered pulpal blood flow,24 and periodontal breakdown.25 The patient also showed a loss of vitality in the maxillary right central incisor and a slight alveolar bone resorption.
The Schwarz appliance is a horseshoe-shaped acrylic appliance that fits along the lingual border of the mandibular dentition, extending to the distal aspect of the permanent second molars. The Schwarz appliance is used typically in patients with mandibular incisor crowding or lingually inclined mandibular posterior teeth.15,26,27 The patient had mandibular incisor crowding and lingually inclined mandibular posterior teeth. Therefore, a decision was made to expand the lower arch with the Schwarz appliance to upright posterior teeth.
Contemporary directional force technology with MIA17 is quite useful, particularly for dentoalveolar protrusion and Class II malocclusion corrections. The key to successful orthodontic treatment is control of the vertical dimensions through anchorage preparation. Control of the horizontal movement of the dentition depends on how the vertical dimensions of the maxillomandibular complex are managed. Vertical control can allow horizontal correction (Fig 11).
A hallmark of Tweed-Merrifield treatment strategy is a directional force system that controls the mandibular anterior and posterior teeth and the maxillary anterior teeth. The resultant vector of all orthodontic forces should be counterclockwise so that the opportunity for a favorable skeletal change is enhanced. Such a force system requires that the mandibular incisors be upright over basal bone so the maxillary incisors can be moved distally and superiorly. For the counterclockwise force system to be a reality, vertical control is critical. To control the vertical dimension, one must control the mandibular plane, the occlusal plane, and the palatal plane. If Point B drops down and back, the face becomes lengthened, the mandibular incisor is tipped forward off basal bone, and the maxillary incisor drops down and back instead of being moved up and back.17,28
Maxillary and mandibular posterior MIs were effective in maintaining or closing the occlusal plane and mandibular plane angle, as well as in inducing forward and upward movement of the chin by intruding the maxillary and mandibular posterior teeth during treatment. In the cephalometric superimposition, intrusion of the maxillary molars was more than the mandibular molars. It can be explained by the different mesio-distal angulation of upper and lower molars. Mandibular molars should be uprighted at the same time as intrusion, and extrusion is inevitable during uprighting. Therefore, the total amount of intrusion of mandibular molars was less than maxillary molars.
Several studies29,30 showed that the center of resistance (CR) of the 6 maxillary anterior teeth was close sagittally and vertically to the cervical one third area of cuspid roots. In en masse retraction, the point of force application is usually above the CR of the upper anterior segment. Therefore, during en masse retraction, uprighting and extrusion of the upper six anterior teeth are inevitable causing a deep bite and a gummy smile. To prevent these detrimental results, intrusive forces can be supplemented in front of the estimated CR of the upper six anterior teeth inducing lingual root torque and intrusion. From this point, maxillary anterior MI is absolutely essential for supporting the maxillary anterior teeth and the anterior segment of the maxilla. Control of the anterior vertical dimensions during treatment inhibits the increase in anterior facial height and allows a large increase in the horizontal mandibular response for a Class II correction, chin enhancement and Z-angle improvement.17
Lee and Park31 reported the relapse rate was 10.36% after intrusion of maxillary posterior teeth and Sugawara et al.32 reported that one third of mandibular molar intrusions relapse during the first year of retention. The patient also showed one third of maxillary molar intrusion relapse during the first year of retention. This is due to the following reasons. One involves the relapse potential that occurs whenever a tooth is intruded. The principal fibers of the periodontal ligament change their orientation and become oblique causing the teeth to extrude.33,34 Another reason is due to the change in facial vertical dimension. Maxillary impaction surgery for correction of skeletal open bite is not stable long-term. A possible reason for instability could be the maxillary osteotomy procedure. But it is due to dentoalveolar changes, not skeletal changes. It seems reasonable that this could be the pattern of physiologic adaptation to the surgery. When the maxilla is moved superiorly, the postural length of the mandibular elevator muscle changes, the mandible rotates upward and forward to a new "rest" (really postural) position, and the freeway space between the posterior teeth remains about the same. Consequently, these would induce clockwise rotation of the mandible and molar extrusion followed by an increase in facial vertical dimension. The tongue posture and hypotonic buccal musculature also can aggravate such relapse.35,36
In this patient, the treatment was successful by reduction of the facial vertical dimension by intrusion of the maxillary and mandibular posterior teeth. The posttreatment changes in the periodontal ligament and mandibular elevator muscle length, and hypotonic musculature are considered as important factors of relapse. In order to prevent relapse of the intruded posterior teeth, a retainer with a posterior bite block was provided, and chewing and nasal breathing exercises were prescribed to strengthen the masticatory muscles and minimize oral breathing.
CONCLUSION
A nasal airway obstruction may be an important factor of arch constriction and long face syndrome. In phase I treatment, correction of the transverse deficiencies was successful by using SARME and Schwarz appliance to expand the constricted arches of the maxilla and mandible caused by the nasal airway obstruction. However, it aggravated the vertical problem. Consequently, in phase II treatment, a contemporary directional force system with MIA was used to control the vertical and horizontal dimensions and an acceptable facial balance was obtained.












 XML Download
XML Download