

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Figures and Tables

 | Fig 2Cast analysis before treatment. There is a mandibular midline deviation of 12.0 mm to the left side and the mandibular arch is asymmetric.
|
 | Fig 3Bone scan results for case 1. Radio-isotope uptake was increased in the right condylar process area.
|
 | Fig 4Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 1.
|
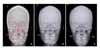
 | Fig 5Posterior-Anterior cephalogram for case 1. A, Before treatment; B, after condylectomy; C, after treatment.
|
 | Fig 6Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 1.
|
 | Fig 7Progressive condyle remodeling on panoramic x-ray for case 1. Four months after condylectomy, twelve months after condylectomy there was a continuous cortical layer on the left condyle. Resected condyle was remodeled in the new position.
|
 | Fig 8Facial and intraoral photographs and panoramic and cephalometric radiographs before treatment for case 2.
|
 | Fig 9Cast analysis before treatment for case 2. It shows mandibular midline deviation of 14.0 mm. There is an occlusal canting with the left side more caudal than the right side.
|
 | Fig 10Bone scan results for case 2. Radio-isotope uptake was increased on the left condylar process area.
|
 | Fig 11Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 2.
|
 | Fig 12Intraoral photograph for molar intrusion and torque control for case 2. Four miniscrews were inserted to intrude molars on the left maxilla buccal and palatal area and a multi loop was used to add buccal crown torque to the right maxilla area.
|
 | Fig 13Facial and intraoral photographs and panoramic and cephalometric radiographs after treatment for case 2.
|
 | Fig 14Posterior-Anterior cephalogram for case 2. A, Before treatment; B, after condylectomy; C, after treatment.
|
 | Fig 15After condylectomy, resected condyle was remodeled in the new position. After five months, condylar shape is getting smoothly rounded, and twenty six months later, it was remodeled to a normal condylar shape.
|

 | Fig 17Principles of condylar hyperplasia treatment. The most important factor to decide is whether the condyle is growing or not to treat the facial asymmetry due to condylar hyperplasia.
|
 | Fig 18Clinical healing pattern after condylectomy. Straight after condylectomy, there is lateral openbite on the unaffected side. According to the remodeling process, lateral openbite is closed and facial asymmetry is improved.
|
 | Fig 19Superimposition of cephalometric tracing of before treatment and after condylectomy (Red: before treatment, Blue: after condylectomy). Molar was intruded and alveolar area was remodeled on the affected area (left side). But there were no changes in the maxillary basal bone area.
|

Table 2

Horizontal, perpendicular to the line passing through crista galli and ANS, which are passing through crista galli; Vertical, line passing through crista galli and ANS; Mx6cusp-horizontal, distance from maxillary first molar palatal cusp to horizontal line; Jugular pc-horizontal, distance from Jugular process to horizontal line; Ag-horizontal, distance from Ag to horizontal line; Menton-vertical, distance from menton to vertical line; Maxilla width, distance between left and right jugular processes; Mandible width, distance between left and right antegonial notches; Ag, antegonial notch.
![]()

Table 4

Horizontal, perpendicular to the vertical line; Vertical, the line passing through crista galli and ANS; Mx6-cusp-horizontal, distance from maxillary first molar palatal cusp to horizontal line; Jugular pc-horizontal, distance from Jugular process to horizontal line; Aghorizontal, distance from Ag to horizontal line; Menton-vertical, distance from menton to vertical line; Maxilla width, distance between left and right jugular processes; Mandible width, distance between left and right antegonial notches; Ag, antegonial notch.
![]()
 XML Download
XML Download