

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
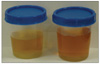
Acute intermittent porphyria (AIP) is a rare disorder characterized biochemically by the increased excretion of porphyrins and porphyrin precursors, including delta-aminolevulinic acid (ALA) and porphobilinogen (PBG). AIP has variable clinical manifestations, such as acute abdominal pain, vomiting, nausea, constipation, peripheral neuropathy, seizures, tachycardia, and hypertension. A 16-year-old girl presented with recurrent abdominal pain, vomiting, hypertension, seizures, hypercholesterolemia, and red urine. AIP was confirmed by clinical features and increased 24-hour urine ALA and PBG. AIP should be considered in the differential diagnosis of patients who have abdominal pain, hypertension, and seizures when the results of all other tests are normal.
Figures and Tables
References
1. Jun DW, Choi CS, Choi HS, Jung YC, Sohn JH, Han DS, et al. A case of acute intermittent porphyria showing respiratory failure and neurologic disorders. Korean J Gastroenterol. 2000. 36:413–418.
2. Kim SH, Chio KY, Park BR. Case reporte: a case report of acute intermittent porphyria. Korean J Intern Med. 1964. 7:377–380.
3. Elder GH, Hift RJ, Meissner PN. The acute porphyrias. Lancet. 1997. 349:1613–1617.

4. Bravenboer B, Erkelens DW. Acute hypertension mimicking phaeochromocytoma as main presenting feature of acute intermittent porphyria. Lancet. 1989. 2:928.
5. Sassa S. Diagnosis and therapy of acute intermittent porphyria. Blood Rev. 1996. 10:53–58.
6. Daniela VA. Acute intermittent porphyria: case report and review of literature. Rev Bras Ter Intensiva. 2008. 20:429–434.
7. Kaplan PW, Lewis DV. Juvenile acute intermittent porphyria with hypercholesterolemia and epilepsy: a case report and review of the literature. J Child Neurol. 1986. 1:38–45.
8. Herrick AL, McColl KE. Acute intermittent porphyria. Best Pract Res Clin Gastroenterol. 2005. 19:235–249.
9. Kauppinen R. Porphyrias. Lancet. 2005. 365:241–252.
10. Andersson C, Lithner F. Hypertension and renal disease in patients with acute intermittent porphyria. J Intern Med. 1994. 236:169–175.
11. Singh V, Sud K, Kohli HS, Gupta KL, Sakhuja V. Acute intermittent porphyria: an unusual cause of malignant hypertension. J Assoc Physicians India. 2003. 51:225–226.
12. Utz N, Kinkel B, Hedde JP, Bewermeyer H. MR imaging of acute intermittent porphyria mimicking reversible posterior leukoencephalopathy syndrome. Neuroradiology. 2001. 43:1059–1062.
13. Maramattom BV, Zaldivar RA, Glynn SM, Eggers SD, Wijdicks EF. Acute intermittent porphyria presenting as a diffuse encephalopathy. Ann Neurol. 2005. 57:581–584.
14. Taddeini L, Frantz I Jr, Sanghvi A. Acceleration of hepatic sterol synthesis after a single dose of the porphyrogenic chemical allylisopropylacetamide. J Lipid Res. 1974. 15:84–88.
15. Whitelaw AG. Acute intermittent porphyria, hypercholesterolaemia, and renal impairment. Arch Dis Child. 1974. 49:406.
16. Fernandez-Miranda C, De La Calle M, Larumbe S, Gomez-Izquierdo T, Porres A, Gomez-Gerique J, et al. Lipoprotein abnormalities in patients with asymptomatic acute porphyria. Clin Chim Acta. 2000. 294:37–43.
17. Schoenfeld N, Mamet R, Lurie Y, Green P, Bomstein Y, Atsmon A. The porphyrinogenic effect of simvastatin in experimental systems. Biomed Pharmacother. 1989. 43:135–139.
 XML Download
XML Download